

Long-term survival after Carpentier-Edwards Perimount aortic valve replacement in Western Denmark: a multi-centre observational study
- PMID: 33990211
- PMCID: PMC8120717
- DOI: 10.1186/s13019-021-01506-x
Long-term survival after Carpentier-Edwards Perimount aortic valve replacement in Western Denmark: a multi-centre observational study
Abstract
Background: This study describes the long-term survival, risk of reoperation and clinical outcomes of patients undergoing solitary surgical aortic valve replacement (SAVR) with a Carpentier-Edwards Perimount (CE-P) bioprosthetic in Western Denmark. The renewed interest in SAVR is based on the questioning regarding the long-term survival since new aortic replacement technique such as transcatheter aortic-valve replacement (TAVR) probably have shorter durability, why assessment of long-term survival could be a key issue for patients.
Methods: From November 1999 to November 2013 a cohort of a total of 1604 patients with a median age of 73 years (IQR: 69-78) undergoing solitary SAVR with CE-P in Western Denmark was obtained November 2018 from the Western Danish Heart Registry (WDHR). The primary endpoint was long-term survival from all-cause mortality. Secondary endpoints were survival free from major adverse cardiovascular and cerebral events (MACCE), risk of reoperation, cause of late death, patient-prothesis mismatch, risk of AMI, stroke, pacemaker or ICD implantation and postoperative atrial fibrillation (POAF). Time-to-event analysis was performed with Kaplan-Meier curve, cumulative incidence function was performed with Nelson-Aalen cumulative hazard estimates. Cox regression was applied to detect risk factors for death and reoperation.
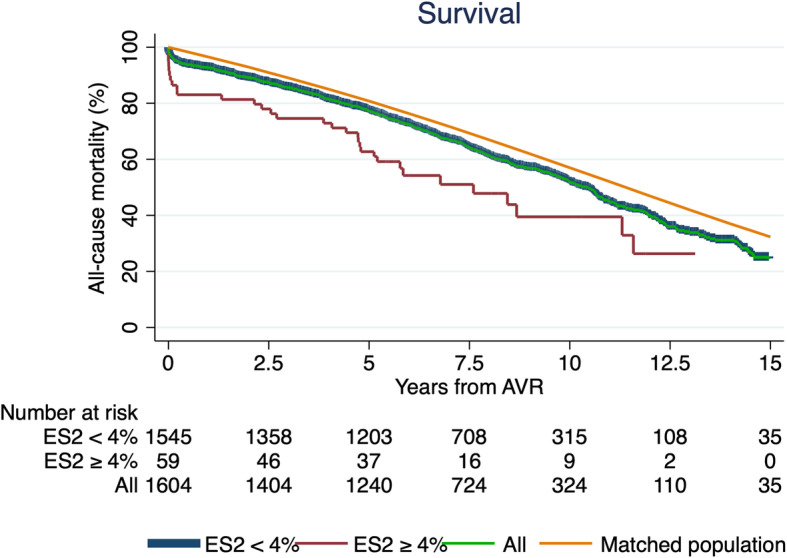
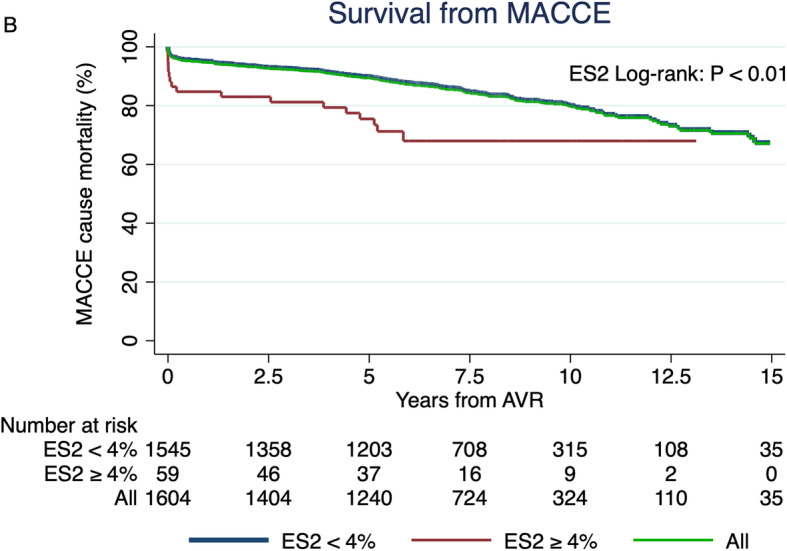
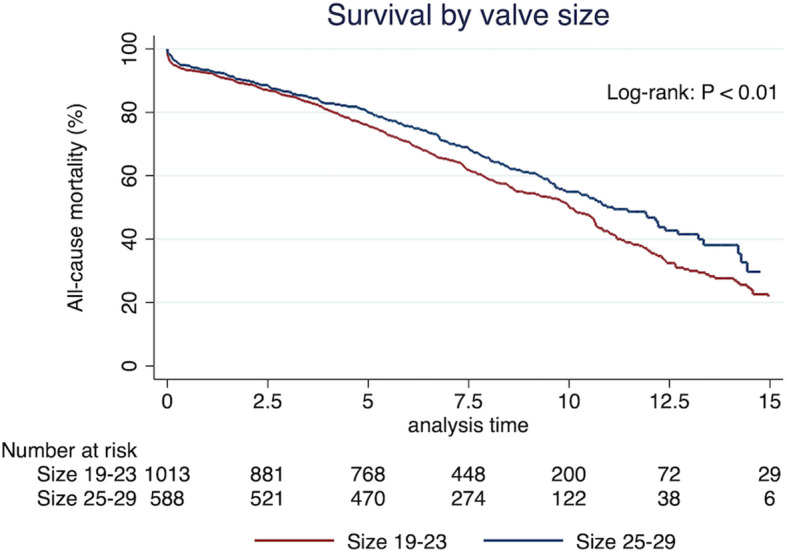
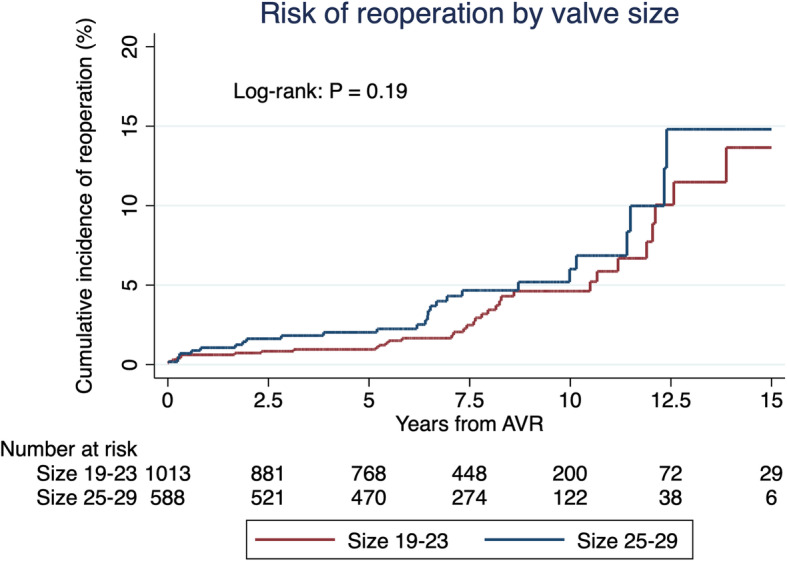
Results: In-hospital mortality was 2.7% and 30-day mortality at 3.4%. The 5-, 10- and 15-year survival from all-cause mortality was 77, 52 and 24%, respectively. Survival without MACCE was 80% after 10 years. Significant risk factors of mortality were small valves, smoking and EuroSCORE II ≥4%. The risk of reoperation was < 5% after 7.5 years and significant risk factors were valve prosthesis-patient mismatch and EuroSCORE II ≥4%.
Conclusions: Patients undergoing aortic valve replacement with a Carpentier-Edwards Perimount valve shows a very satisfying long-term survival. Future research should aim to investigate biological valves long-term durability for comparison of different SAVR to different TAVR in long perspective.
Keywords: Aortic valve replacement; Carpentier-Edwards Perimount; Long-term survival.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Baumgartner H, Falk V, Bax JJ, de Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Rodriguez Muñoz D, Rosenhek R, Sjögren J, Tornos Mas P, Vahanian A, Walther T, Wendler O, Windecker S, Zamorano JL, ESC Scientific Document Group. Roffi M, Alfieri O, Agewall S, Ahlsson A, Barbato E, Bueno H, Collet JP, Coman IM, Czerny M, Delgado V, Fitzsimons D, Folliguet T, Gaemperli O, Habib G, Harringer W, Haude M, Hindricks G, Katus HA, Knuuti J, Kolh P, Leclercq C, McDonagh TA, Piepoli MF, Pierard LA, Ponikowski P, Rosano GMC, Ruschitzka F, Shlyakhto E, Simpson IA, Sousa-Uva M, Stepinska J, Tarantini G, Tchétché D, Aboyans V, Windecker S, Aboyans V, Agewall S, Barbato E, Bueno H, Coca A, Collet JP, Coman IM, Dean V, Delgado V, Fitzsimons D, Gaemperli O, Hindricks G, Iung B, Jüni P, Katus HA, Knuuti J, Lancellotti P, Leclercq C, McDonagh T, Piepoli MF, Ponikowski P, Richter DJ, Roffi M, Shlyakhto E, Simpson IA, Zamorano JL, Kzhdryan HK, Mascherbauer J, Samadov F, Shumavets V, Camp GV, Lončar D, Lovric D, Georgiou GM, Linhartova K, Ihlemann N, Abdelhamid M, Pern T, Turpeinen A, Srbinovska-Kostovska E, Cohen A, Bakhutashvili Z, Ince H, Vavuranakis M, Temesvári A, Gudnason T, Mylotte D, Kuperstein R, Indolfi C, Pya Y, Bajraktari G, Kerimkulova A, Rudzitis A, Mizariene V, Lebrun F, Demarco DC, Oukerraj L, Bouma BJ, Steigen TK, Komar M, de Moura Branco LM, Popescu BA, Uspenskiy V, Foscoli M, Jovovic L, Simkova I, Bunc M, de Prada JAV, Stagmo M, Kaufmann BA, Mahdhaoui A, Bozkurt E, Nesukay E, Brecker SJD. 2017 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739–2791. doi: 10.1093/eurheartj/ehx391. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
