

Use of historical high-sensitivity cardiac troponin T levels to rule out myocardial infarction
- PMID: 33990434
- PMCID: PMC8127977
- DOI: 10.1136/openhrt-2021-001682
Use of historical high-sensitivity cardiac troponin T levels to rule out myocardial infarction
Abstract
Objective: Several high-sensitivity cardiac troponin (hs-cTn)-based strategies exist for rule-out of myocardial infarction (MI). It is unknown whether historical hs-cTnT concentrations can be used. This study aim to evaluate the performance of a rule-out strategy based on the European Society of Cardiology (ESC) 0/1-hour algorithm, using historical hs-cTnT concentrations.
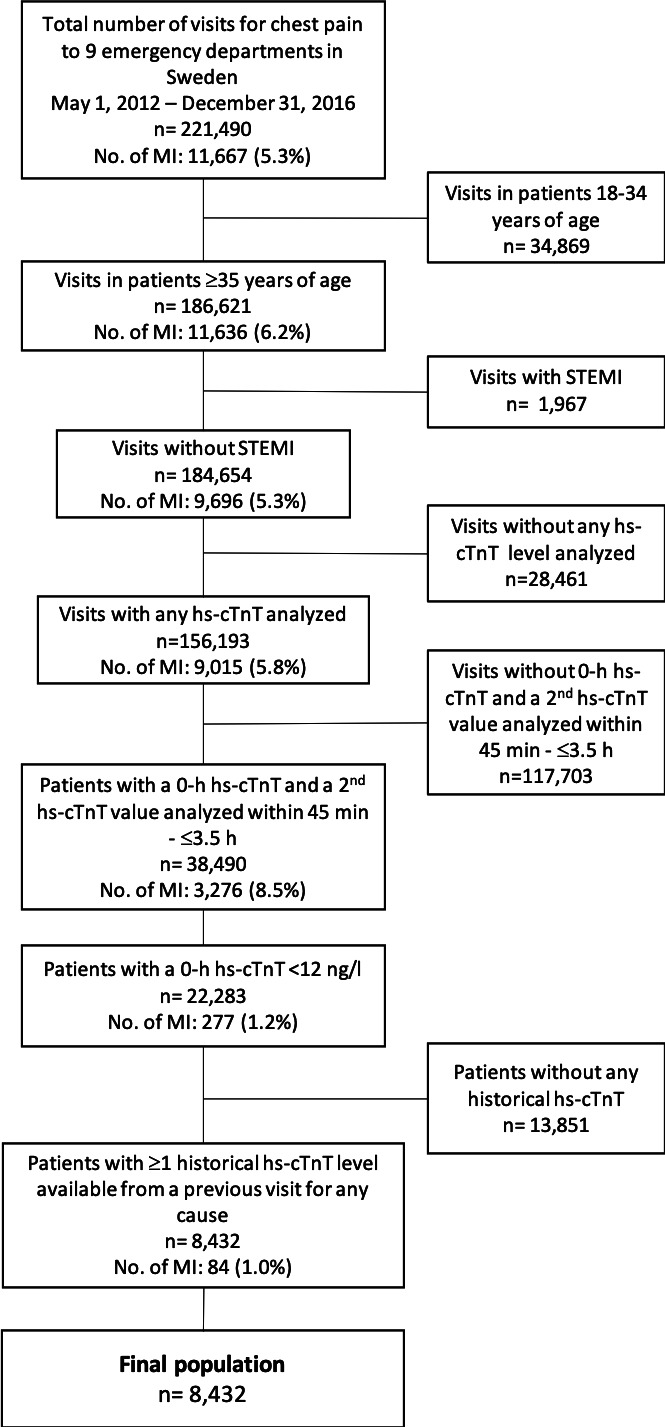
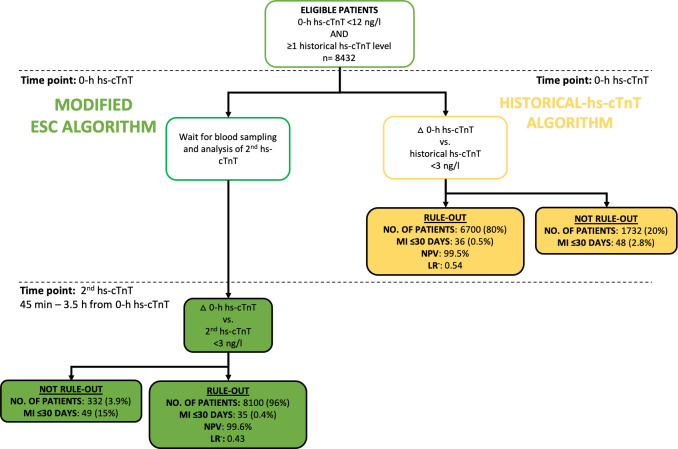
Methods: All visits among patients with chest pain in the emergency department at nine different hospitals in Sweden from 2012 to 2016 were eligible (221 490 visits). We enrolled patients with a 0-hour hs-cTnT of <12 ng/L, a second hs-cTnT measured within 3.5 hours, and ≥1 historical hs-cTnT available. We calculated the risks of MI and all-cause mortality using two rule-out strategies: (1) a delta hs-cTnT of <3 ng/L between the 0-hour hs-cTnT and the second hs-cTnT (modified ESC algorithm) and (2) a historical hs-cTnT <12 ng/L and a delta hs-cTnT of <3 ng/L in relation to the 0-hour hs-cTnT (historical-hs-cTnT algorithm).
Results: A total of 8432 patients were included, of whom 84 (1.0%) had an MI. The modified ESC algorithm triaged 8100 (96%) patients toward ruled-out, for whom 30-day MI risk and negative predictive value (NPV) for MI (95% CI) were 0.4% (0.3% to 0.6%) and 99.6% (99.4% to 99.7%), respectively. The historical-hs-cTnT algorithm ruled out 6700 (80%) patients, with a 30-day MI risk of 0.5% (0.4% to 0.8%) and NPV of 99.5% (99.2% to 99.6%).
Conclusions: The application of algorithm resulted in similar MI risk and NPV to an established algorithm. The usefulness of historical hs-cTnT concentrations should merit further attention.
Keywords: biomarkers; chest pain; myocardial infarction.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MJH has received consultancy honoraria from Idorsia and Pfizer.
Figures
Similar articles
-
Undetectable high-sensitivity cardiac troponin T level in the emergency department and risk of myocardial infarction.J Am Coll Cardiol. 2014 Jun 17;63(23):2569-2578. doi: 10.1016/j.jacc.2014.03.017. Epub 2014 Mar 30. J Am Coll Cardiol. 2014. PMID: 24694529
-
European Society of Cardiology 0/1-hour algorithm (high-sensitivity cardiac troponin T) performance across distinct age groups.Heart. 2024 May 23;110(12):838-845. doi: 10.1136/heartjnl-2023-323621. Heart. 2024. PMID: 38471727
-
Combining High-Sensitivity Cardiac Troponin I and Cardiac Troponin T in the Early Diagnosis of Acute Myocardial Infarction.Circulation. 2018 Sep 4;138(10):989-999. doi: 10.1161/CIRCULATIONAHA.117.032003. Circulation. 2018. PMID: 29691270
-
Safety and efficacy of the European Society of Cardiology 0/1-hour algorithm for diagnosis of myocardial infarction: systematic review and meta-analysis.Heart. 2020 Jul;106(13):985-991. doi: 10.1136/heartjnl-2019-316343. Epub 2020 Apr 3. Heart. 2020. PMID: 32245882
-
Serial high-sensitivity cardiac troponin T measurements to rule out acute myocardial infarction and a single high baseline measurement for swift rule-in: A systematic review and meta-analysis.Eur Heart J Acute Cardiovasc Care. 2020 Feb;9(1):14-22. doi: 10.1177/2048872618819421. Epub 2019 Jan 8. Eur Heart J Acute Cardiovasc Care. 2020. PMID: 30618277 Free PMC article.
Cited by
-
Using historical cardiac troponins to identify patients at a high risk of myocardial infarction.Heart. 2022 Dec 22;109(2):127-133. doi: 10.1136/heartjnl-2022-321198. Heart. 2022. PMID: 35948410 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous