

An ensemble of neural networks provides expert-level prenatal detection of complex congenital heart disease
- PMID: 33990806
- PMCID: PMC8380434
- DOI: 10.1038/s41591-021-01342-5
An ensemble of neural networks provides expert-level prenatal detection of complex congenital heart disease
Abstract
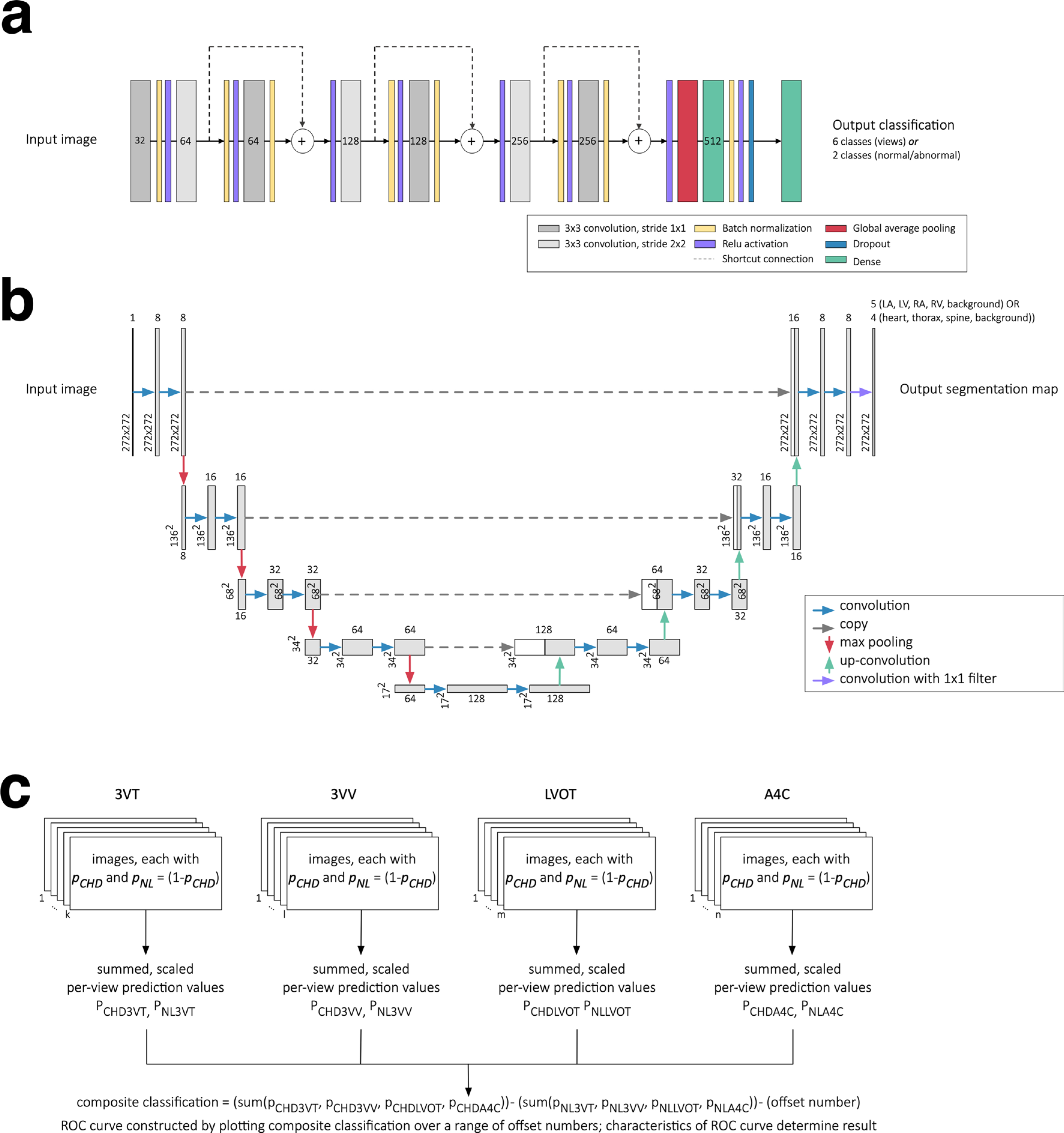
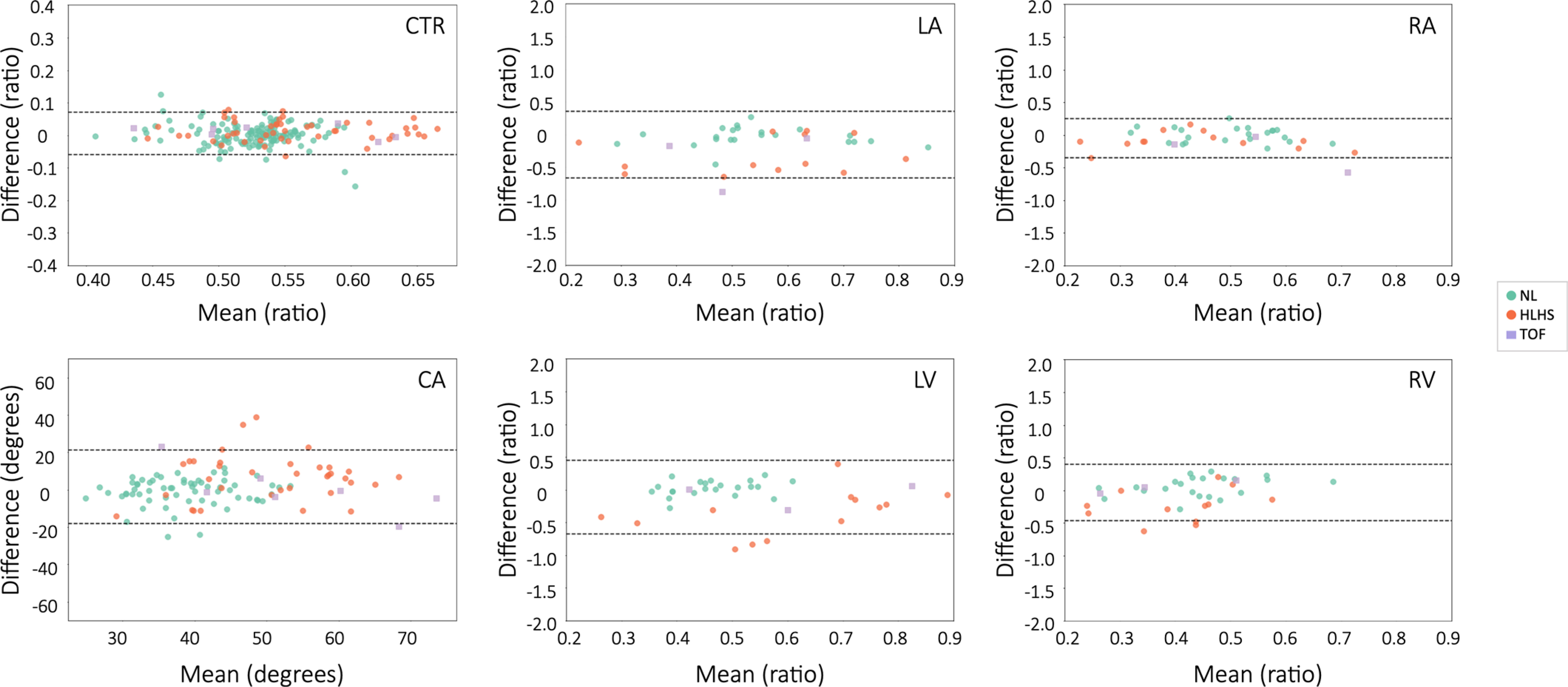
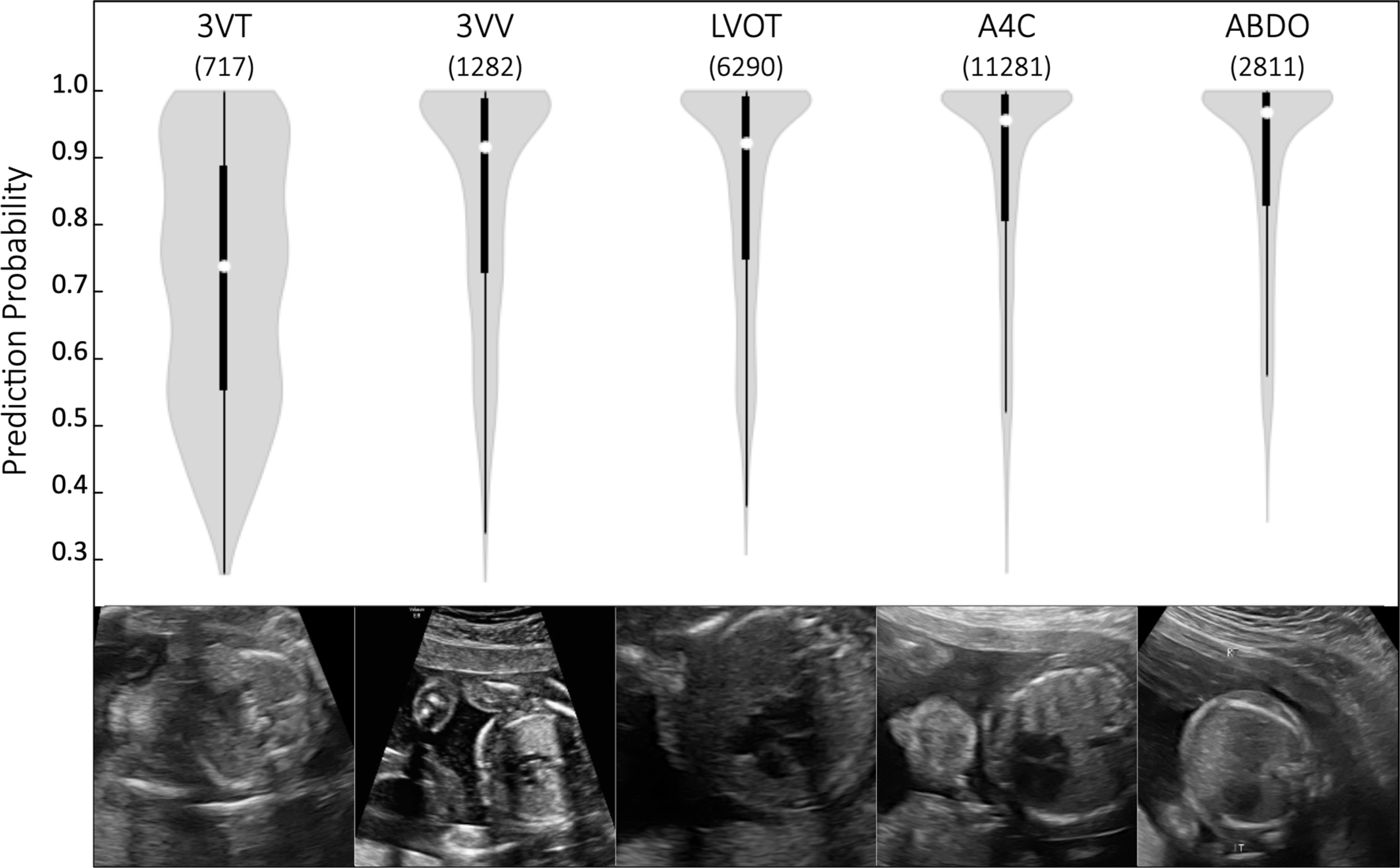
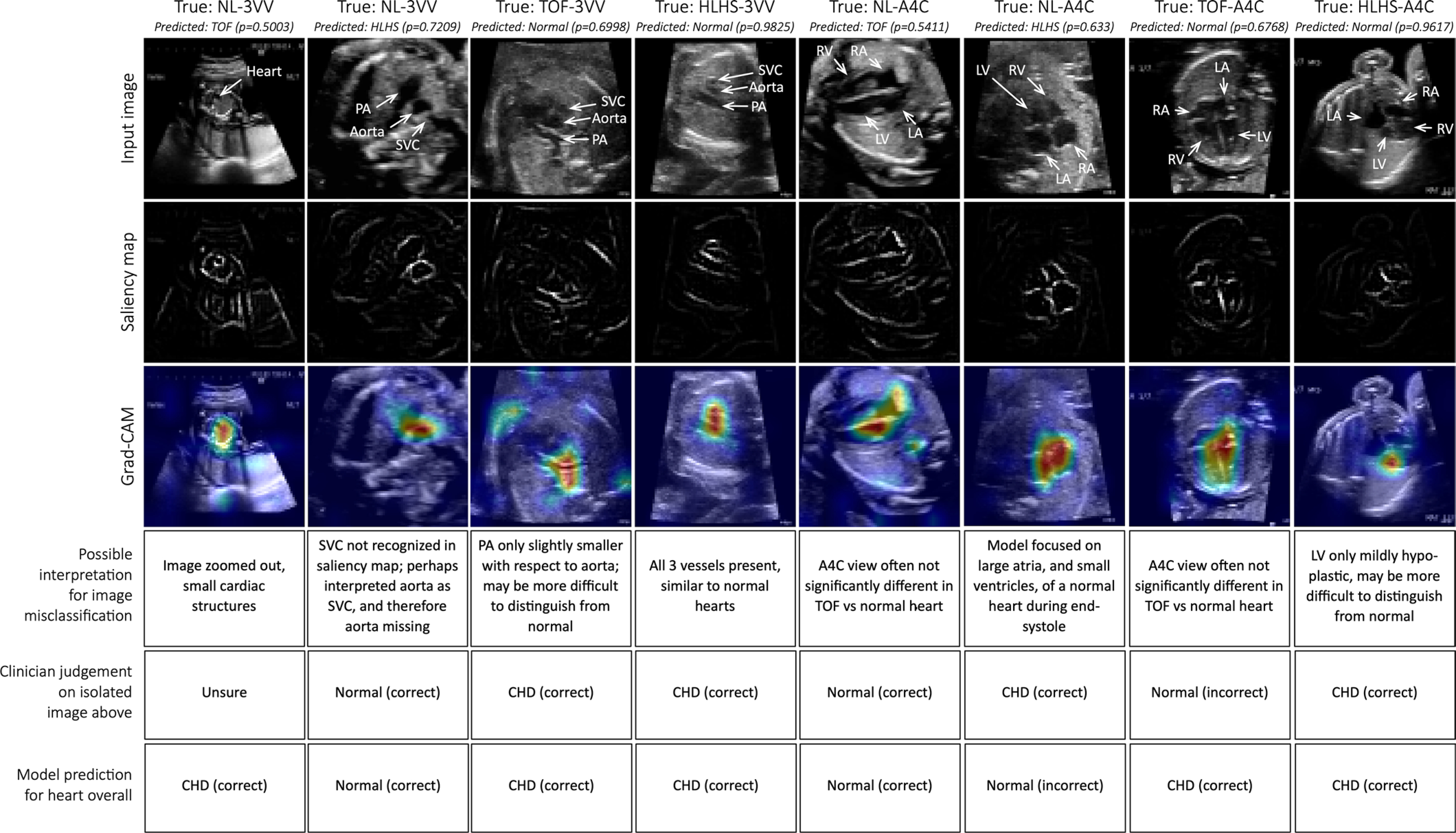
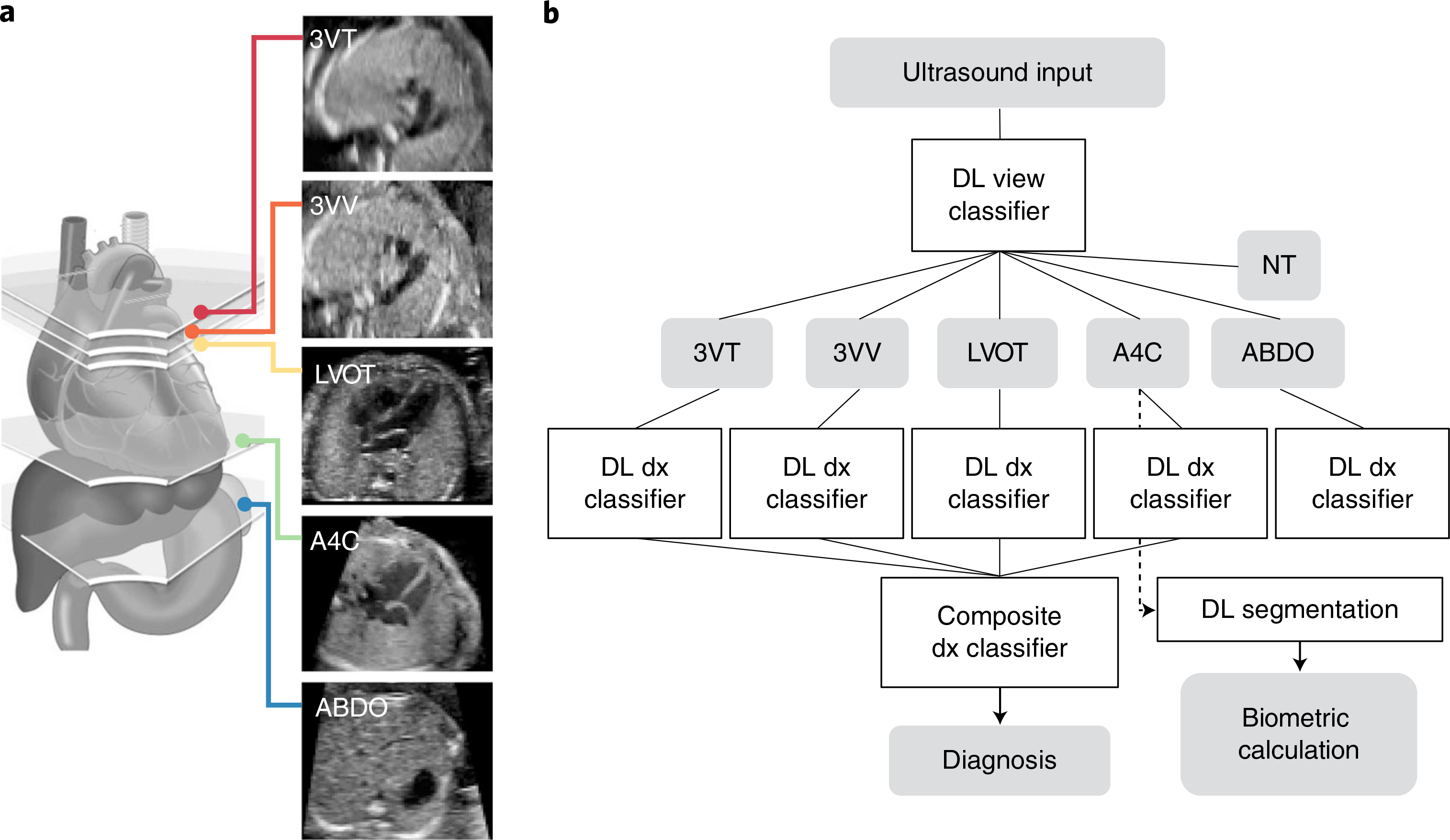
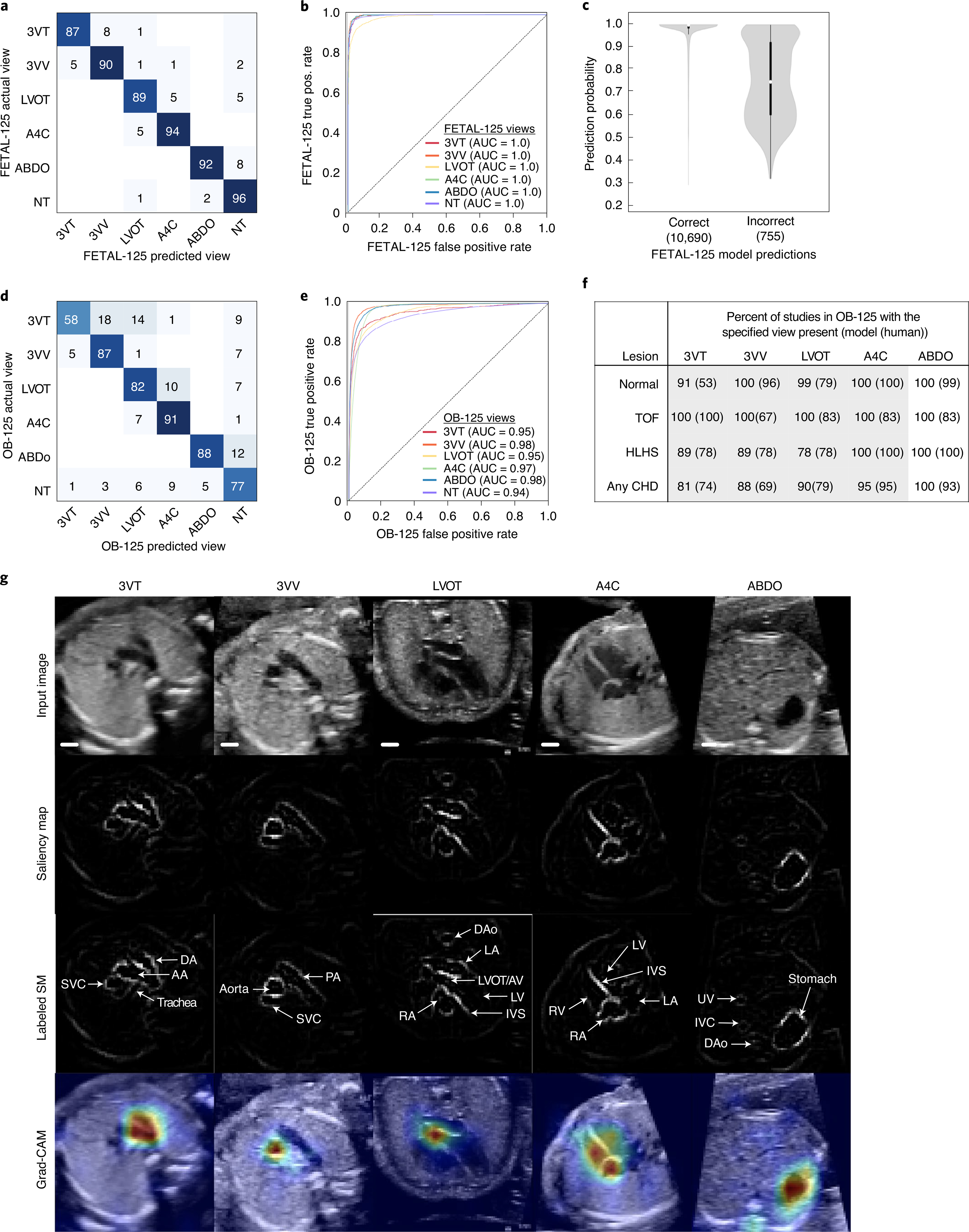
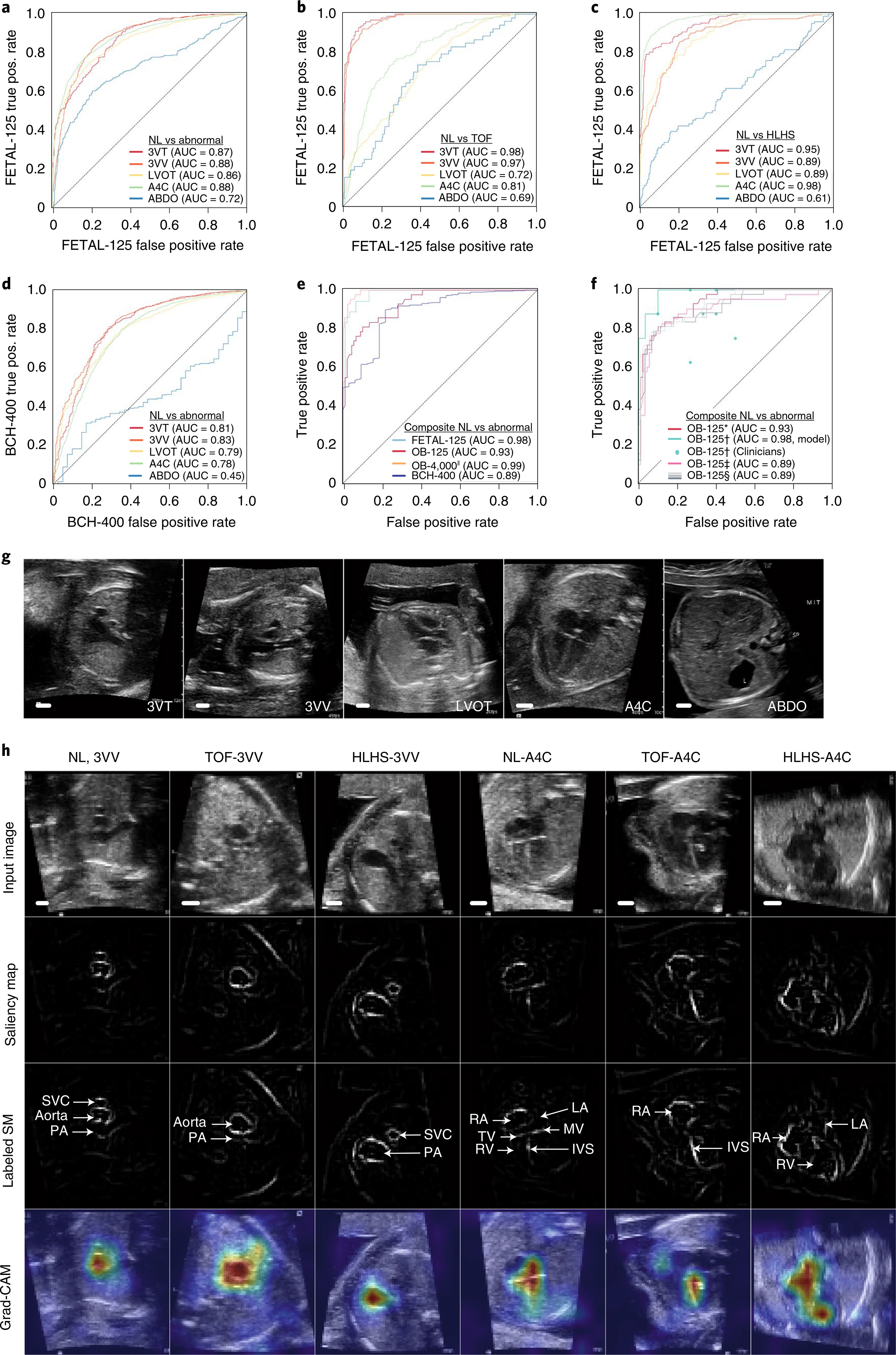
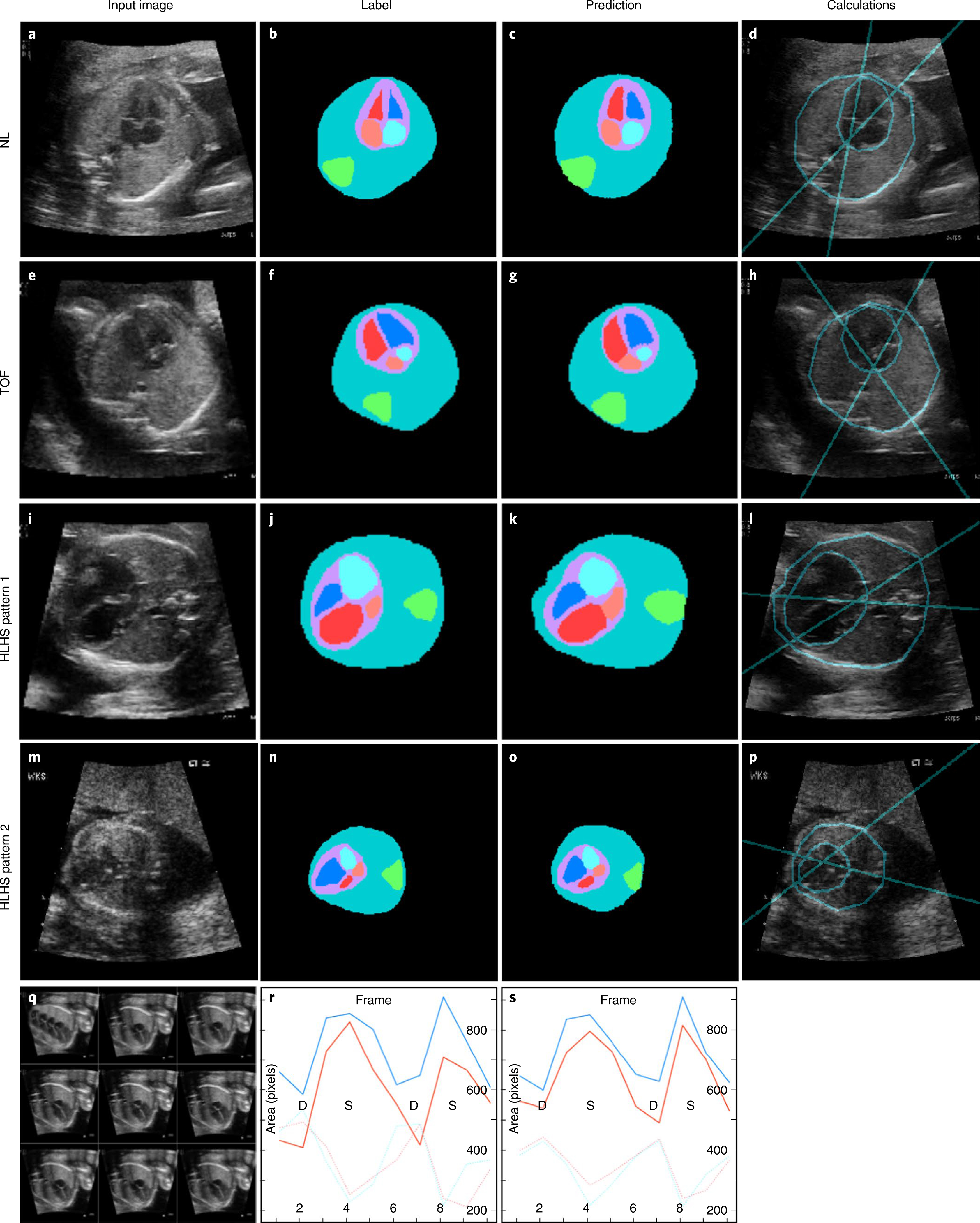
Congenital heart disease (CHD) is the most common birth defect. Fetal screening ultrasound provides five views of the heart that together can detect 90% of complex CHD, but in practice, sensitivity is as low as 30%. Here, using 107,823 images from 1,326 retrospective echocardiograms and screening ultrasounds from 18- to 24-week fetuses, we trained an ensemble of neural networks to identify recommended cardiac views and distinguish between normal hearts and complex CHD. We also used segmentation models to calculate standard fetal cardiothoracic measurements. In an internal test set of 4,108 fetal surveys (0.9% CHD, >4.4 million images), the model achieved an area under the curve (AUC) of 0.99, 95% sensitivity (95% confidence interval (CI), 84-99%), 96% specificity (95% CI, 95-97%) and 100% negative predictive value in distinguishing normal from abnormal hearts. Model sensitivity was comparable to that of clinicians and remained robust on outside-hospital and lower-quality images. The model's decisions were based on clinically relevant features. Cardiac measurements correlated with reported measures for normal and abnormal hearts. Applied to guideline-recommended imaging, ensemble learning models could significantly improve detection of fetal CHD, a critical and global diagnostic challenge.
Conflict of interest statement
Competing interests
Some methods used in this work have been filed in a provisional patent application.
Figures
Comment in
-
Deep learning for detecting congenital heart disease in the fetus.Nat Med. 2021 May;27(5):764-765. doi: 10.1038/s41591-021-01354-1. Nat Med. 2021. PMID: 33990805 No abstract available.
Similar articles
-
Deep-learning model for prenatal congenital heart disease screening generalizes to community setting and outperforms clinical detection.Ultrasound Obstet Gynecol. 2024 Jan;63(1):44-52. doi: 10.1002/uog.27503. Ultrasound Obstet Gynecol. 2024. PMID: 37774040 Free PMC article.
-
The added value of screening fetal echocardiography after normal cardiac views on a detailed ultrasound.Prenat Diagn. 2019 Nov;39(12):1148-1154. doi: 10.1002/pd.5557. Epub 2019 Sep 13. Prenat Diagn. 2019. PMID: 31499581
-
Length to width ratio of the ductus venosus in simple screening for fetal congenital heart diseases in the second trimester.Medicine (Baltimore). 2016 Sep;95(39):e4928. doi: 10.1097/MD.0000000000004928. Medicine (Baltimore). 2016. PMID: 27684831 Free PMC article.
-
Fetal cardiac screening: 1st trimester and beyond.Prenat Diagn. 2024 Jun;44(6-7):679-687. doi: 10.1002/pd.6571. Epub 2024 Apr 12. Prenat Diagn. 2024. PMID: 38613152 Review.
-
Prenatal diagnosis of congenital heart disease: A review of current knowledge.Indian Heart J. 2018 Jan-Feb;70(1):150-164. doi: 10.1016/j.ihj.2017.12.005. Epub 2017 Dec 16. Indian Heart J. 2018. PMID: 29455772 Free PMC article. Review.
Cited by
-
The Lifelong Impact of Artificial Intelligence and Clinical Prediction Models on Patients With Tetralogy of Fallot.CJC Pediatr Congenit Heart Dis. 2023 Aug 29;2(6Part A):440-452. doi: 10.1016/j.cjcpc.2023.08.005. eCollection 2023 Dec. CJC Pediatr Congenit Heart Dis. 2023. PMID: 38161675 Free PMC article. Review.
-
Can Artificial Intelligence Revolutionize the Diagnosis and Management of the Atrial Septal Defect in Children?Diagnostics (Basel). 2024 Jan 6;14(2):132. doi: 10.3390/diagnostics14020132. Diagnostics (Basel). 2024. PMID: 38248009 Free PMC article. Review.
-
Machine learning and disease prediction in obstetrics.Curr Res Physiol. 2023 May 19;6:100099. doi: 10.1016/j.crphys.2023.100099. eCollection 2023. Curr Res Physiol. 2023. PMID: 37324652 Free PMC article. Review.
-
Ensemble of fine-tuned machine learning models for hysterectomy prediction in pregnant women using magnetic resonance images.J Med Imaging (Bellingham). 2025 Mar;12(2):024502. doi: 10.1117/1.JMI.12.2.024502. Epub 2025 Mar 18. J Med Imaging (Bellingham). 2025. PMID: 40109885
-
Recent advances and applications of artificial intelligence in 3D bioprinting.Biophys Rev (Melville). 2024 Jul 19;5(3):031301. doi: 10.1063/5.0190208. eCollection 2024 Sep. Biophys Rev (Melville). 2024. PMID: 39036708 Free PMC article. Review.
References
-
- Donofrio MT et al.Diagnosis and treatment of fetal cardiac disease: a scientific statement from the American Heart Association. Circulation 129, 2183–2242 (2014). - PubMed
-
- Holland BJ, Myers JA & Woods CR Jr. Prenatal diagnosis of critical congenital heart disease reduces risk of death from cardiovascular compromise prior to planned neonatal cardiac surgery: a meta-analysis. Ultrasound Obstet. Gynecol. 45, 631–638 (2015). - PubMed
-
- Wright LK et al.Relation of prenatal diagnosis with one-year survival rate for infants with congenital heart disease. Am. J. Cardiol. 113, 1041–1044 (2014). - PubMed
-
- Bensemlali M et al.Neonatal management and outcomes of prenatally diagnosed CHDs. Cardiol. Young 27, 344–353 (2017). - PubMed
-
- Li YF et al.Efficacy of prenatal diagnosis of major congenital heart disease on perinatal management and perioperative mortality: a meta-analysis. World J. Pediatr. 12, 298–307 (2016). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
