

High-risk individuals for gastric cancer would be missed for surveillance without subtyping of intestinal metaplasia
- PMID: 33990867
- PMCID: PMC8740520
- DOI: 10.1007/s00428-021-03116-3
High-risk individuals for gastric cancer would be missed for surveillance without subtyping of intestinal metaplasia
Abstract
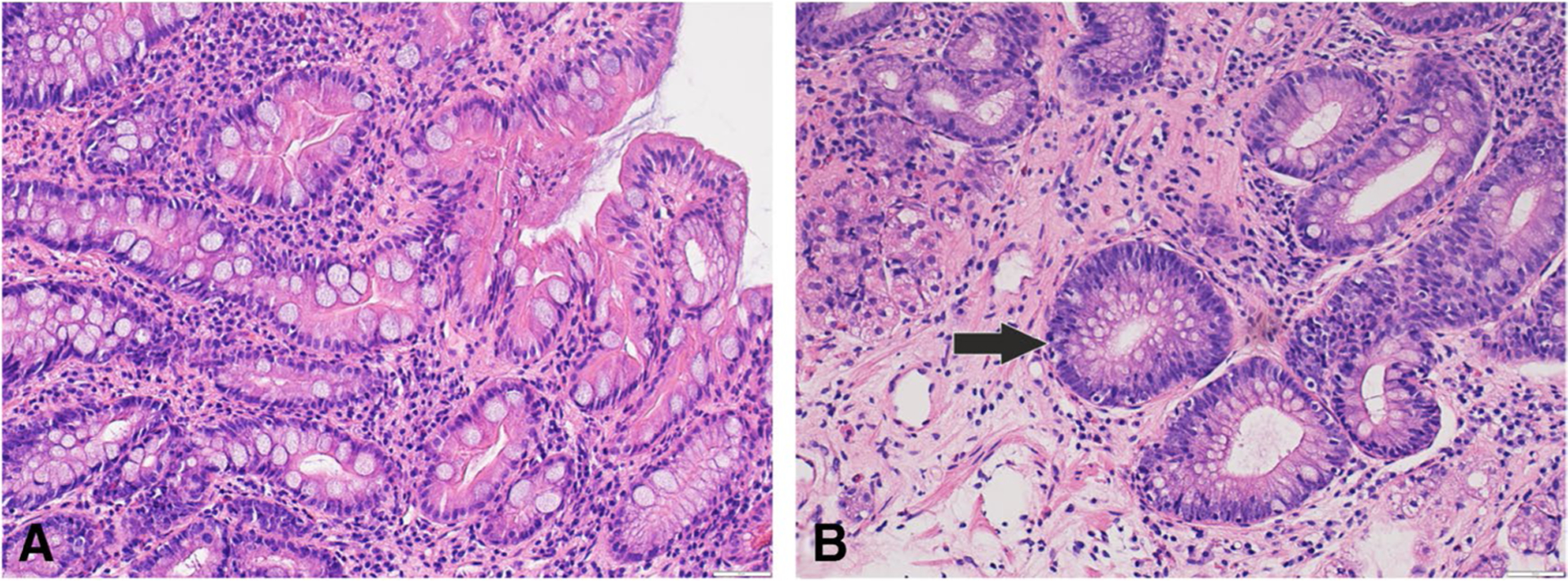
The use of Operative Link on Gastritis Assessment (OLGA) and Operative Link on Gastritis Assessment based on Intestinal Metaplasia (OLGIM) staging system is recommended for identifying subjects at risk for developing gastric cancer; usually high-risk lesions are considered only as stages III and IV. Accumulating evidence suggests that incomplete intestinal metaplasia (IM) is important in the development of gastric cancer. Our aim has been to identify the prevalence of incomplete IM in patients with low-risk OLGA/OLGIM stages among a high-risk general population. Healthy adult volunteers aged 40-64 years were invited to undergo upper endoscopy within a regional GISTAR pilot study in Kazakhstan (n = 166). Gastric lesions were staged according to OLGA/OLGIM staging system. High iron diamine-alcian blue (HID-AB) was used for subtyping IM. IM prevalence overall was 45.8%. Incomplete IM was present in 52.6% (type II in 30.3% and type III in 22.3%), whereas complete IM was found in 47.4% individuals. The prevalence of OLGIM I and II stage were 39.8 and 4.8%, respectively, whereas OLGIM III was observed in 1.2%. The prevalence of incomplete IM in patients stratified to OLGIM I was 54.5% (type II in 31.8% and type III in 22.7%). High prevalence of incomplete IM was detected not only in subjects with extensive IM, but in those stratified as at the OLGIM I stage. Without IM subtyping, patients with high risk of gastric cancer development would be missed for surveillance.
Keywords: Gastric cancer; OLGA; OLGIM intestinal metaplasia; Risk stratification; Subtypes.
© 2021. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
Figures

References
-
- Pimentel-Nunes P, Libanio D, Marcos-Pinto R et al. (2019) Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update. Endoscopy 51(4):365–388. 10.1055/a-0859-1883 - DOI - PubMed
-
- Rugge M, Correa P, Dixon MF, Fiocca R, Hattori T, Lechago J, Leandro G, Price AB, Sipponen P, Solcia E, Watanabe H, Genta RM (2002) Gastric mucosal atrophy: interobserver consistency using new criteria for classification and grading. Pharmacol Ther 16(7):1249–1259. 10.1046/j.1365-2036.2002.01301.x - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
