

High Prevalence of Anal High-Grade Squamous Intraepithelial Lesions, and Prevention Through Human Papillomavirus Vaccination, in Young Men Who Have Sex With Men Living With Human Immunodeficiency Virus
- PMID: 33991185
- PMCID: PMC8528397
- DOI: 10.1093/cid/ciab434
High Prevalence of Anal High-Grade Squamous Intraepithelial Lesions, and Prevention Through Human Papillomavirus Vaccination, in Young Men Who Have Sex With Men Living With Human Immunodeficiency Virus
Abstract
Background: Men who have sex with men (MSM) are at high risk for human papillomavirus (HPV)-related anal cancer. Little is known about the prevalence of low-grade squamous intraepithelial lesions (LSILs) and the anal cancer precursor, high-grade squamous intraepithelial lesions (HSILs), among young MSM with HIV (MSMLWH). HPV vaccination is recommended in this group, but its safety, immunogenicity, and protection against vaccine-type HPV infection and associated LSILs/HSILs have not been studied.
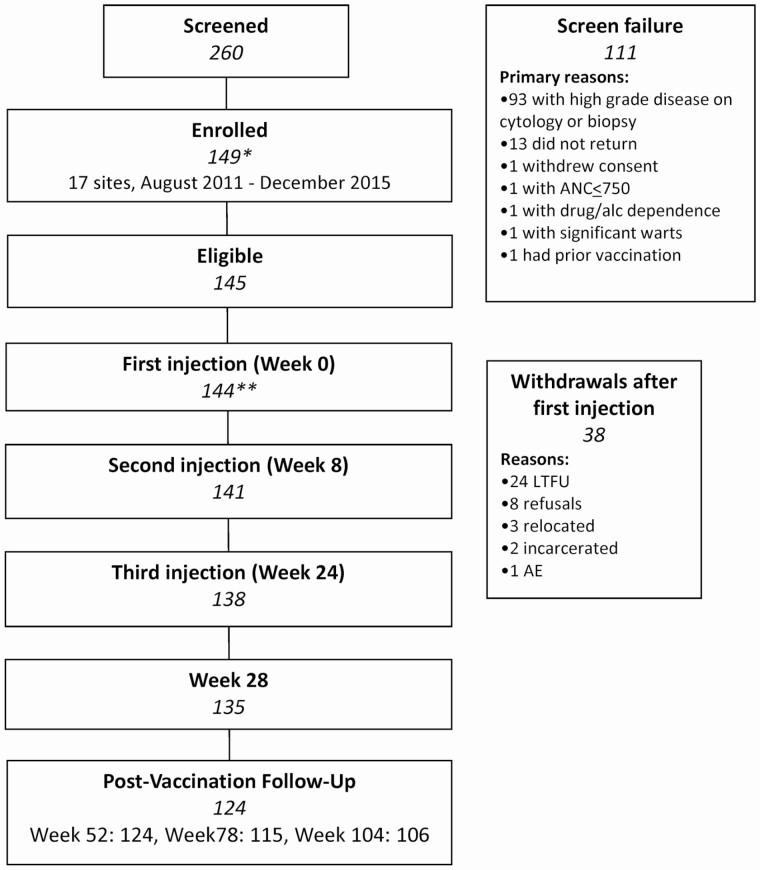
Methods: Two hundred and sixty MSMLWH aged 18-26 years were screened at 17 US sites for a clinical trial of the quadrivalent (HPV6,11,16,18) HPV (qHPV) vaccine. Those without HSILs were vaccinated at 0, 2, and 6 months. Cytology, high-resolution anoscopy with biopsies of lesions, serology, and HPV testing of the mouth/penis/scrotum/anus/perianus were performed at screening/month 0 and months 7, 12, and 24.
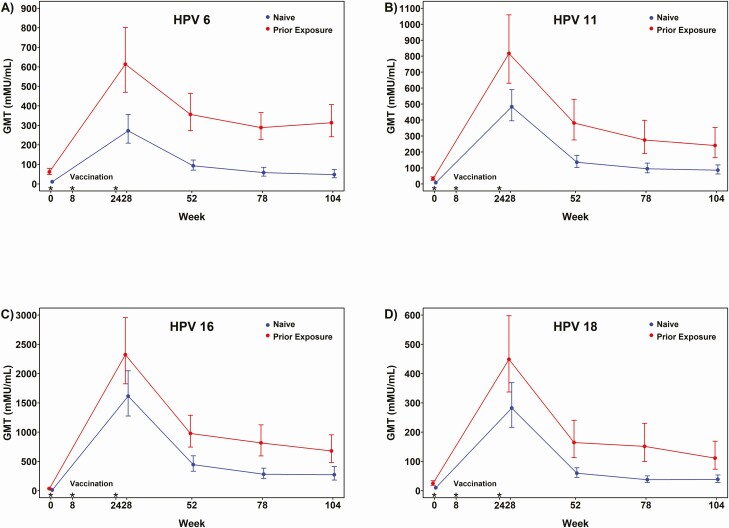
Results: Among 260 MSMLWH screened, the most common reason for exclusion was detection of HSILs in 88/260 (34%). 144 MSMLWH were enrolled. 47% of enrollees were previously exposed to HPV16. No incident qHPV type-associated anal LSILs/HSILs were detected among men naive to that type, compared with 11.1, 2.2, 4.5, and 2.8 cases/100 person-years for HPV6,11,16,18-associated LSILs/HSILs, respectively, among those previously exposed to that type. qHPV was immunogenic and safe with no vaccine-associated serious adverse events.
Conclusions: 18-26-year-old MSMLWH naive to qHPV vaccine types were protected against incident qHPV type-associated LSILs/HSILs. Given their high prevalence of HSILs, there is an urgent need to vaccinate young MSMLWH before exposure to vaccine HPV types, before initiating sexual activity, and to perform catch-up vaccination.
Keywords: anal human papillomavirus infection; anal squamous intraepithelial lesions; human immunodeficiency virus; men who have sex with men; quadrivalent HPV vaccine.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Palefsky JM, Giuliano AR, Goldstone S, et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N Engl J Med 2011; 365:1576–85. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
