

Direct comparison of risankizumab and fumaric acid esters in systemic therapy-naïve patients with moderate-to-severe plaque psoriasis: a randomized controlled trial
- PMID: 33991341
- PMCID: PMC9291944
- DOI: 10.1111/bjd.20481
Direct comparison of risankizumab and fumaric acid esters in systemic therapy-naïve patients with moderate-to-severe plaque psoriasis: a randomized controlled trial
Abstract
Background: Fumaric acid esters (FAEs; Fumaderm® ) are the most frequently prescribed first-line systemic treatment for moderate-to-severe plaque psoriasis in Germany. Risankizumab (Skyrizi® ) is a humanized IgG1 monoclonal antibody that specifically binds to the p19 subunit of interleukin 23.
Objectives: To compare risankizumab treatment to FAEs in patients with psoriasis.
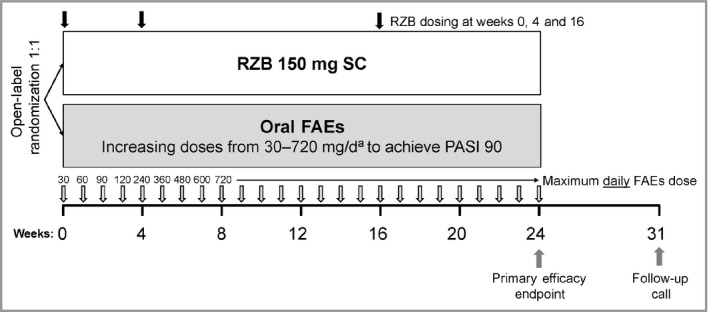
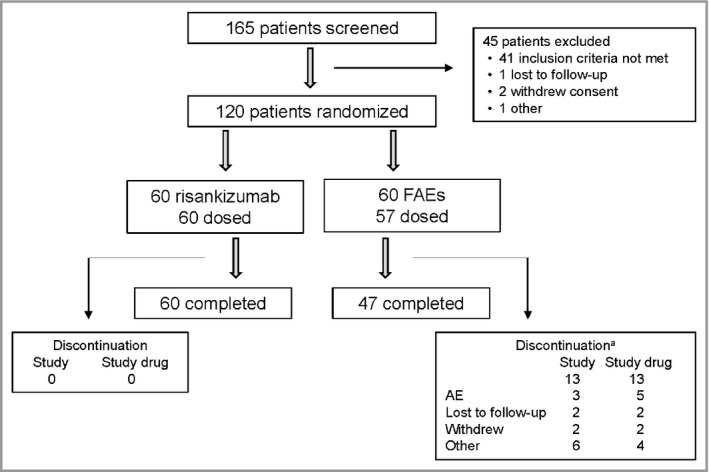
Methods: This phase III randomized, active-controlled, open-label study with blinded assessment of efficacy was conducted in Germany. Patients were randomized (1 : 1) to subcutaneous risankizumab 150 mg (weeks 0, 4 and 16) or oral FAEs at increasing doses from 30 mg daily (week 0) up to 720 mg daily (weeks 8-24). Enrolled patients were adults naïve to and candidates for systemic therapy, with chronic moderate-to-severe plaque psoriasis. Phototherapy was not allowed within 14 days before or during the study.
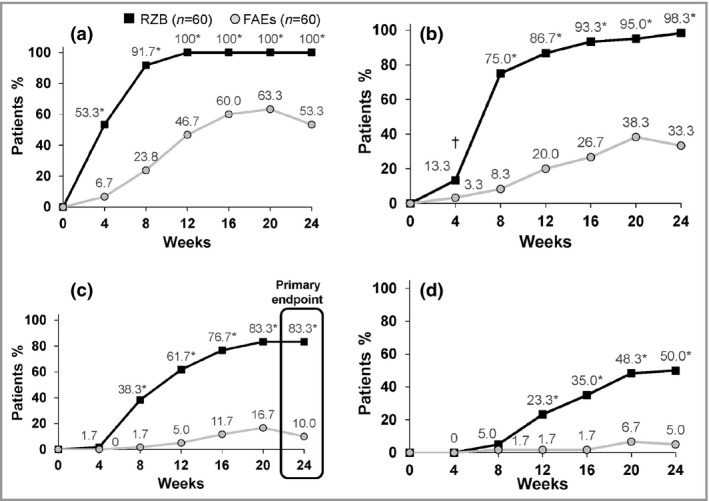
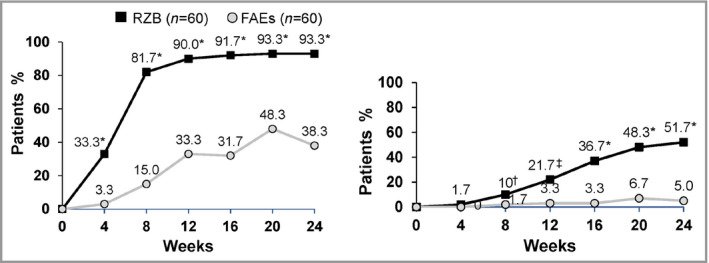
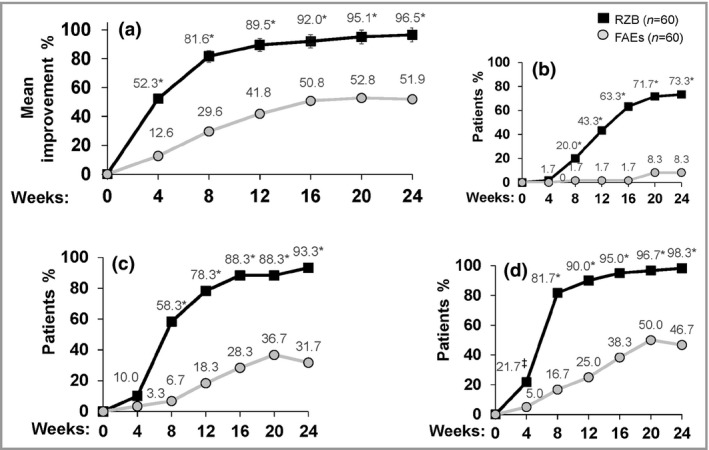
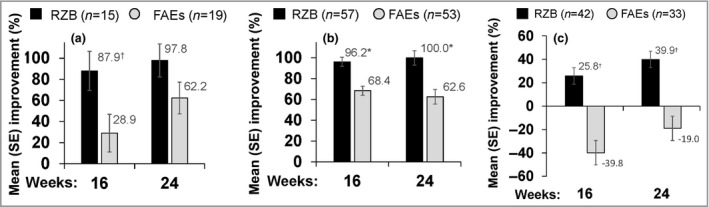
Results: Key efficacy endpoints were met at week 24 for risankizumab (n = 60) vs. FAEs (n = 60) (P < 0·001): achievement of a ≥ 90% improvement in Psoriasis Area and Severity Index (PASI; primary endpoint 83·3% vs. 10·0%), ≥ 100% improvement in PASI (50·0% vs. 5·0%), ≥ 75% improvement in PASI (98·3% vs. 33·3%), ≥ 50% improvement in PASI (100% vs. 53·3%) and a Static Physician's Global Assessment of clear/almost clear (93·3% vs. 38·3%). The rates of gastrointestinal disorders, flushing, lymphopenia and headache were higher in the FAE group. One patient receiving risankizumab reported a serious infection (influenza, which required hospitalization). There were no malignancies, tuberculosis or opportunistic infections in either treatment arm.
Conclusions: Risankizumab was found to be superior to FAEs, providing earlier and greater improvement in psoriasis outcomes that persisted with continued treatment, and more favourable safety results, which is consistent with the known safety profile. No new safety signals for risankizumab or FAEs were observed.
© 2021 The Authors. British Journal of Dermatology published by John Wiley & Sons Ltd on behalf of British Association of Dermatologists.
Figures
Comment in
-
Risankizumab vs. fumaric acid esters: a direct comparison.Br J Dermatol. 2022 Jan;186(1):4-5. doi: 10.1111/bjd.20813. Epub 2021 Nov 2. Br J Dermatol. 2022. PMID: 34726768 No abstract available.
References
-
- Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med 2009; 361:496–509. - PubMed
-
- Lowes MA, Bowcock AM, Krueger JG. Pathogenesis and therapy of psoriasis. Nature 2007; 445:866–73. - PubMed
-
- Parisi R, Symmons DP, Griffiths CE et al. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol 2013; 133:377–85. - PubMed
-
- Menter A, Griffiths CE. Current and future management of psoriasis. Lancet 2007; 370:272–84. - PubMed
-
- Goff KL, Karimkhani C, Boyers LN et al. The global burden of psoriatic skin disease. Br J Dermatol 2015; 172:1665–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
