

Comparative efficacy and safety of systemic therapies used in moderate-to-severe atopic dermatitis: a systematic literature review and network meta-analysis
- PMID: 33991374
- PMCID: PMC8453983
- DOI: 10.1111/jdv.17351
Comparative efficacy and safety of systemic therapies used in moderate-to-severe atopic dermatitis: a systematic literature review and network meta-analysis
Abstract
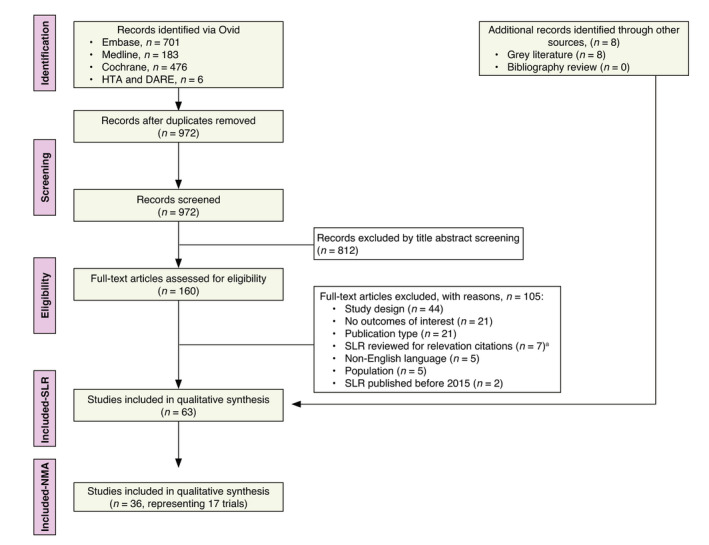
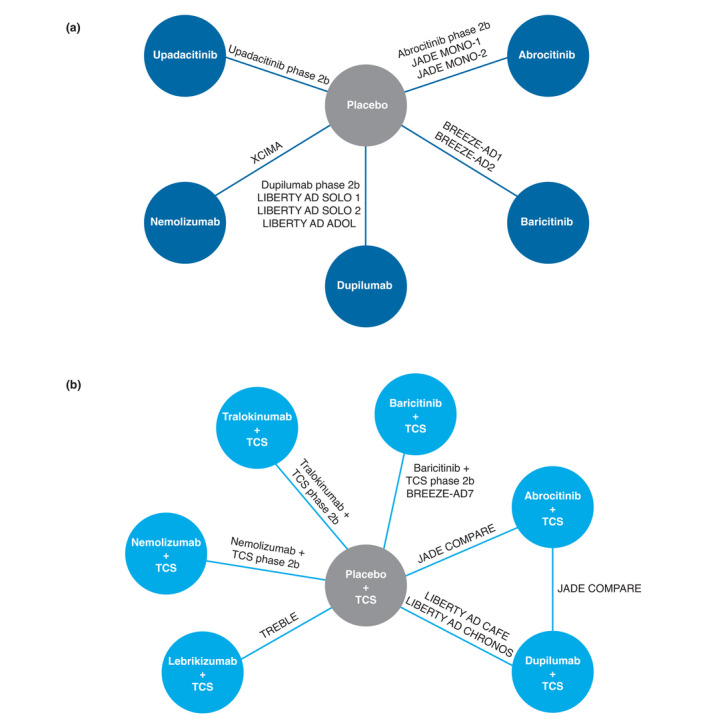
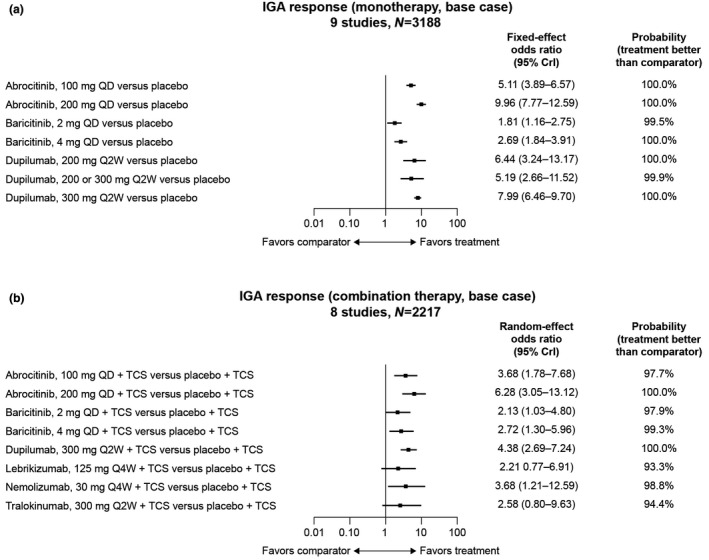
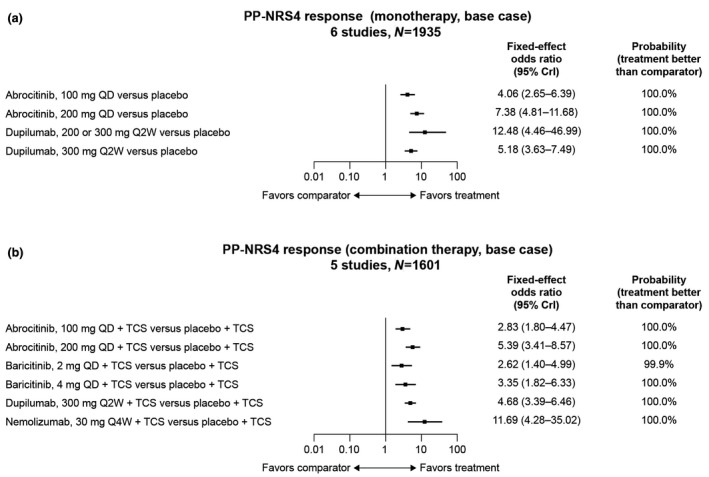
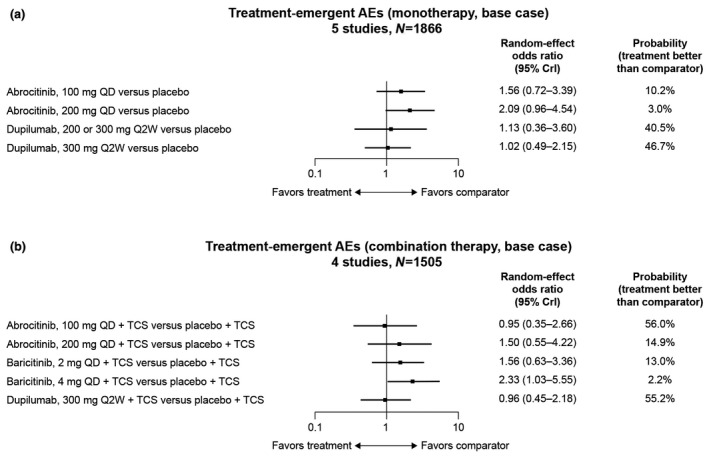
Given the lack of head-to-head studies of systemic therapies in moderate-to-severe atopic dermatitis (AD), network meta-analyses (NMAs) can provide comparative efficacy and safety data to inform clinical decision-making. In this NMA, eligible randomized controlled trials (RCTs) published before 24 October 2019 were identified by a systematic literature review. Short-term (12-16 weeks) efficacy (Investigator's Global Assessment [IGA] and Eczema Area and Severity Index [EASI] responses), patient-reported outcomes (PROs) and safety data from each trial were abstracted and analysed separately for monotherapy and combination therapy (systemic plus topical anti-inflammatory therapy). RCTs were analysed in fixed-effects and random-effects Bayesian NMA models. Overall, 19 phase 2 and phase 3 RCTs of abrocitinib, baricitinib, dupilumab, lebrikizumab, nemolizumab, tralokinumab and upadacitinib were included. In monotherapy RCTs, upadacitinib 30 mg once daily (QD) had the numerically highest efficacy (83.6% achieved ≥50% improvement in EASI [EASI-50 response]), followed by abrocitinib 200 mg QD (74.6%), upadacitinib 15 mg QD (70.5%), dupilumab 300 mg every 2 weeks (Q2W) (63.4%) and abrocitinib 100 mg QD (56.7%). Similar trends in EASI-75 and EASI-90 response were observed. In combination therapy RCTs, abrocitinib 200 mg QD had the highest EASI-50 (86.6%), followed by dupilumab 300 mg Q2W (82.4%) and abrocitinib 100 mg QD (79.7%). Similar findings were observed for IGA response and PROs. In monotherapy and combination therapy RCTs, the probability of treatment-emergent adverse events (TEAEs) was higher among all active treatments than with placebo (except for dupilumab 300 mg Q2W [odds ratio (OR), 0.96; 95% credible interval (CrI), 0.45-2.18] and abrocitinib 100 mg QD [OR, 0.95; 95% CrI, 0.35-2.66] in combination therapy RCTs), although active treatments did not significantly differ from one another. Abrocitinib, dupilumab and upadacitinib were consistently the most effective systemic therapies in adult and adolescent patients with AD, with no significant TEAE differences in short-term RCTs.
© 2021 Pfizer Inc. Journal of the European Academy of Dermatology and Venereology published by John Wiley & Sons Ltd on behalf of European Academy of Dermatology and Venereology.
Figures
References
-
- Boguniewicz M, Fonacier L, Guttman‐Yassky E, Ong PY, Silverberg J, Farrar JR. Atopic dermatitis yardstick: Practical recommendations for an evolving therapeutic landscape. Ann Allergy Asthma Immunol 2018; 120: 10–22.e12. - PubMed
-
- Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet 2020; 396: 345–360. - PubMed
-
- DaVeiga SP. Epidemiology of atopic dermatitis: a review. Allergy Asthma Proc 2012; 33: 227–234. - PubMed
-
- Silverberg JI, Hanifin JM. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population‐based study. J Allergy Clin Immunol 2013; 132: 1132–1138. - PubMed
-
- Eckert L, Gupta S, Amand C, Gadkari A, Mahajan P, Gelfand JM. Impact of atopic dermatitis on health‐related quality of life and productivity in adults in the United States: An analysis using the National Health and Wellness Survey. J Am Acad Dermatol 2017; 77: 274–279.e273. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
