

Prior ischemic strokes are non-inferior for predicting future ischemic strokes than CHA2DS2-VASc score in hemodialysis patients with non-valvular atrial fibrillation
- PMID: 33992086
- PMCID: PMC8126112
- DOI: 10.1186/s12882-021-02384-0
Prior ischemic strokes are non-inferior for predicting future ischemic strokes than CHA2DS2-VASc score in hemodialysis patients with non-valvular atrial fibrillation
Abstract
Background: We tested whether CHA2DS2-VASc and/or HAS-BLED scores better predict ischemic stroke and major bleeding, respectively, than their individual components in maintenance hemodialysis (MHD) patients with atrial fibrillation (AF).
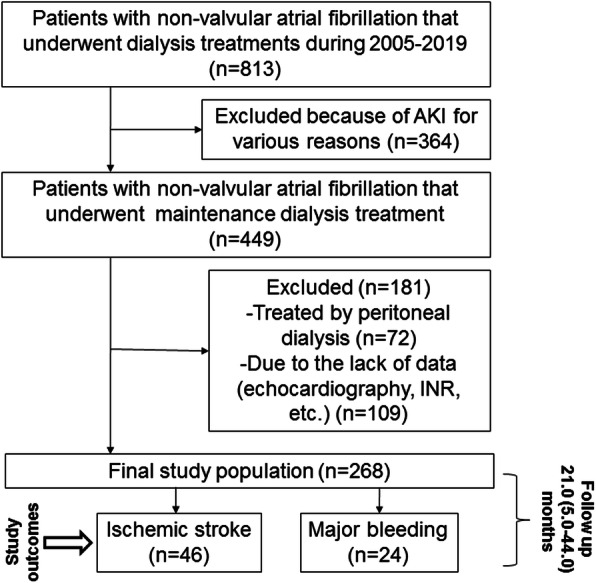
Methods: A retrospective cohort study of a clinical database containing the medical records of 268 MHD patients with non-valvular AF (167 women, mean age 73.4 ± 10.2 years). During the median follow-up of 21.0 (interquartile range, 5.0-44.0) months, 46 (17.2%) ischemic strokes and 24 (9.0%) major bleeding events were reported.
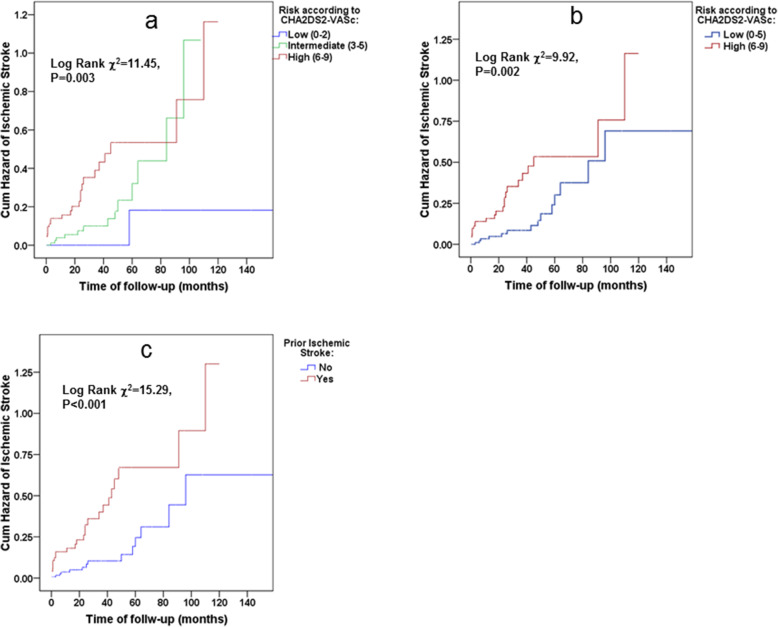
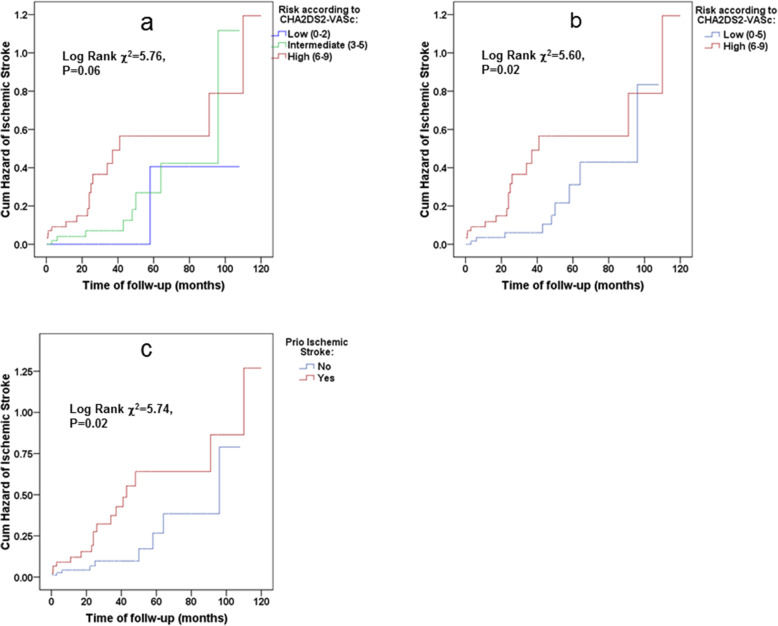
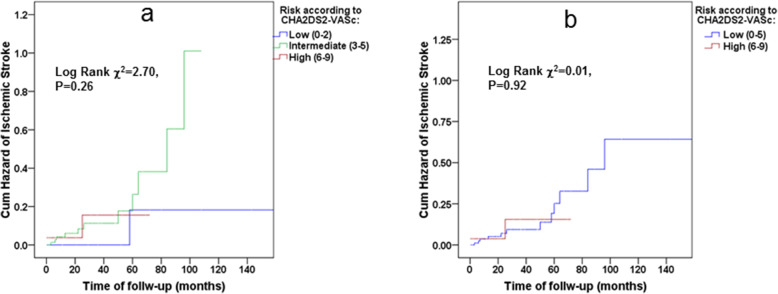
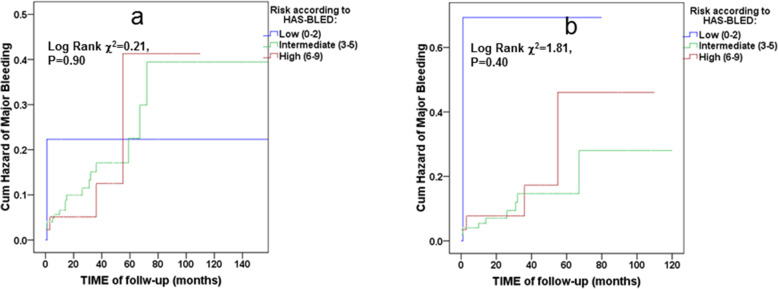
Results: Although CHA2DS2-VASc predicted ischemic stroke risk in the study population (adjusted HR 1.74 with 95% CI 1.23-2.46 for each unit of increase in CHA2DS2-VASc score, and HR of 5.57 with 95% CI 1.88-16.49 for CHA2DS2-VASc score ≥ 6), prior ischemic strokes/transient ischemic attacks (TIAs) were non-inferior in both univariate and multivariate analyses (adjusted HR 8.65 with 95% CI 2.82-26.49). The ROC AUC was larger for the prior ischemic stroke/TIA than for CHA2DS2-VASc. Furthermore, the CHA2DS2-VASc score did not predict future ischemic stroke risks in study participants who did not previously experience ischemic strokes/TIAs (adjusted HR 1.41, 95% CI: 0.84-2.36). The HAS-BLED score and its components did not have predictive abilities in discriminating bleeding risk in the study population.
Conclusions: Previous ischemic strokes are non-inferior for predicting of future ischemic strokes than the complete CHA2DS2-VASc score in MHD patients. CHA2DS2VASc scores are less predictive in MHD patients without histories of CVA/TIA. HAS-BLED scores do not predict major bleeding in MHD patients. These findings should redesign approaches to ischemic stroke risk stratification in MHD patients if future large-scale epidemiological studies confirm them.
Keywords: Bleeding; CHA2DS2-VASc; HAS-BLED; Hemodialysis; Stroke.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Dynamic assessment of CHA2DS2-VASc and HAS-BLED scores for predicting ischemic stroke and major bleeding in atrial fibrillation patients.Rev Esp Cardiol (Engl Ed). 2024 Oct;77(10):835-842. doi: 10.1016/j.rec.2024.02.011. Epub 2024 Mar 7. Rev Esp Cardiol (Engl Ed). 2024. PMID: 38460882 English, Spanish.
-
The HAS-BLED score has better prediction accuracy for major bleeding than CHADS2 or CHA2DS2-VASc scores in anticoagulated patients with atrial fibrillation.J Am Coll Cardiol. 2013 Dec 10;62(23):2199-204. doi: 10.1016/j.jacc.2013.08.1623. Epub 2013 Sep 18. J Am Coll Cardiol. 2013. PMID: 24055744
-
CHADS2 and CHA2DS2-VASc Scores Predict the Risk of Ischemic Stroke Outcome in Patients with Interatrial Block without Atrial Fibrillation.J Atheroscler Thromb. 2017 Feb 1;24(2):176-184. doi: 10.5551/jat.34900. Epub 2016 Jun 15. J Atheroscler Thromb. 2017. PMID: 27301462 Free PMC article.
-
Diagnostic Accuracy of the HAS-BLED Bleeding Score in VKA- or DOAC-Treated Patients With Atrial Fibrillation: A Systematic Review and Meta-Analysis.Front Cardiovasc Med. 2021 Nov 22;8:757087. doi: 10.3389/fcvm.2021.757087. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34881309 Free PMC article.
-
Utility of the CHA2DS2-VASc score for predicting ischaemic stroke in patients with or without atrial fibrillation: a systematic review and meta-analysis.Eur J Prev Cardiol. 2022 Mar 30;29(4):625-631. doi: 10.1093/eurjpc/zwab018. Eur J Prev Cardiol. 2022. PMID: 33693717
Cited by
-
Comprehensive comparison of stroke risk score performance: a systematic review and meta-analysis among 6 267 728 patients with atrial fibrillation.Europace. 2022 Nov 22;24(11):1739-1753. doi: 10.1093/europace/euac096. Europace. 2022. PMID: 35894866 Free PMC article.
-
Application of computed tomographic angiography and echocardiography in predicting left atrial appendage thrombosis in patients with non-valvular atrial fibrillation.Cardiovasc J Afr. 2023 Sep-Oct 23;34(4):231-236. doi: 10.5830/CVJA-2022-052. Epub 2022 Nov 16. Cardiovasc J Afr. 2023. PMID: 36383152 Free PMC article.
-
Use of Neutrophil-to-Lymphocyte Ratio to Predict In-Hospital Mortality in Patients Admitted with Acute Decompensation of Atrial Fibrillation.J Clin Med. 2024 Aug 12;13(16):4719. doi: 10.3390/jcm13164719. J Clin Med. 2024. PMID: 39200861 Free PMC article.
-
Cardiovascular Events and Mortality in Patients on Hemodialysis: The Prognostic Value of the CHA2DS2-VASc Score.Medicina (Kaunas). 2024 Jan 12;60(1):144. doi: 10.3390/medicina60010144. Medicina (Kaunas). 2024. PMID: 38256404 Free PMC article.
References
-
- Baber U, Howard VJ, Halperin JL, Soliman EZ, Zhang X, McClellan W, Warnock DG, Muntner P. Association of chronic kidney disease with atrial fibrillation among adults in the United States: REasons for geographic and racial differences in stroke (REGARDS) study. Circ Arrhythm Electrophysiol. 2011;4(1):26–32. doi: 10.1161/CIRCEP.110.957100. - DOI - PMC - PubMed
-
- Buiten MS, de Bie MK, Rotmans JI, Gabreëls BA, van Dorp W, Wolterbeek R, Trines SA, Schalij MJ, Jukema JW, Rabelink TJ, van Erven L. The dialysis procedure as a trigger for atrial fibrillation: new insights in the development of atrial fibrillation in dialysis patients. Heart. 2014;100(9):685–690. doi: 10.1136/heartjnl-2013-305417. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
