

Mild traumatic brain injury increases vulnerability to cerebral ischemia in mice
- PMID: 33992581
- PMCID: PMC8210428
- DOI: 10.1016/j.expneurol.2021.113765
Mild traumatic brain injury increases vulnerability to cerebral ischemia in mice
Abstract
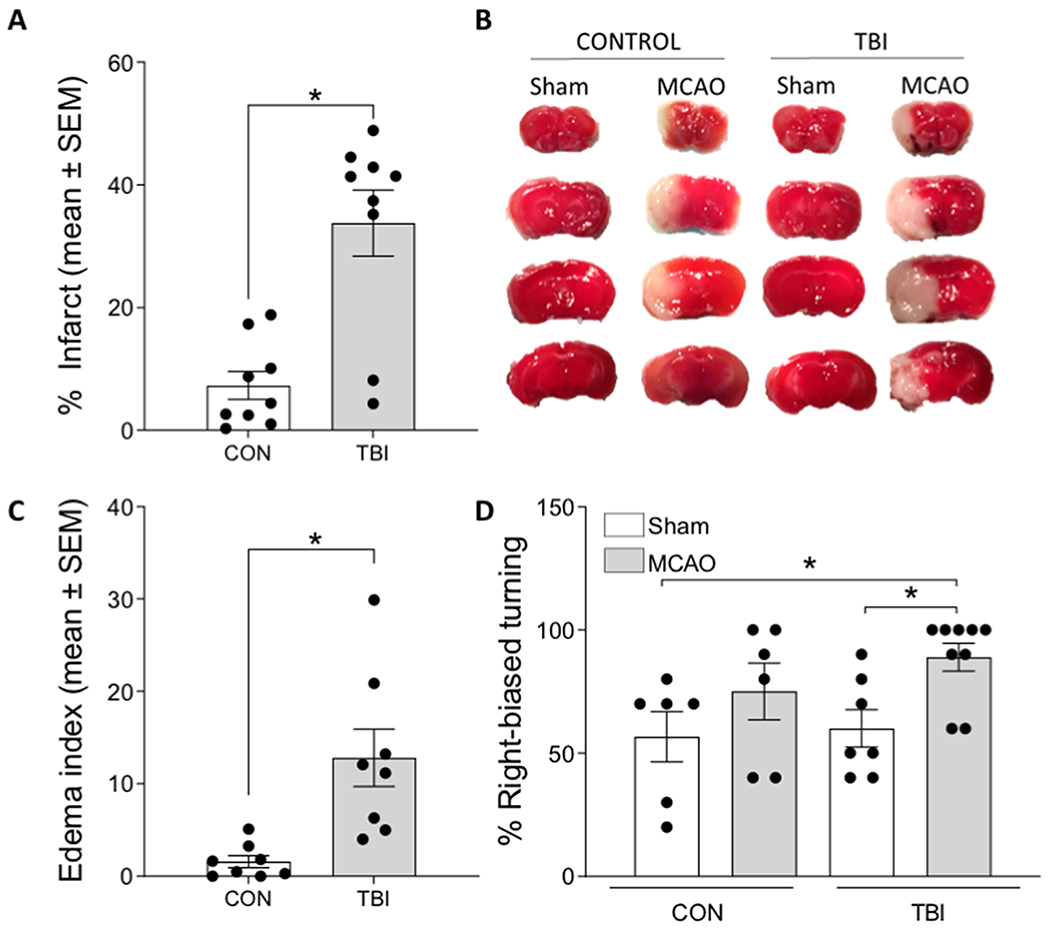
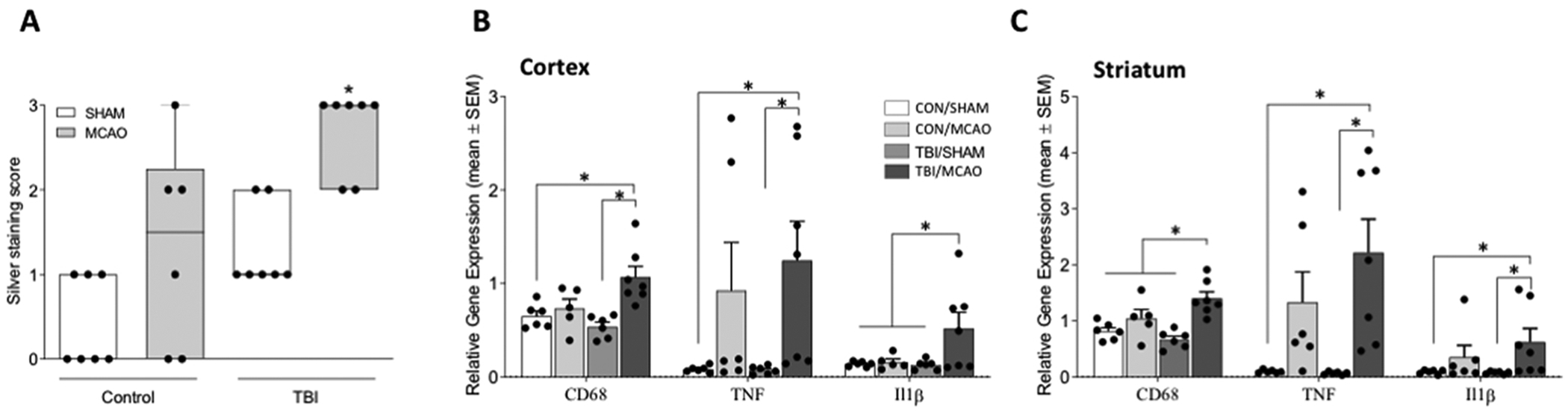
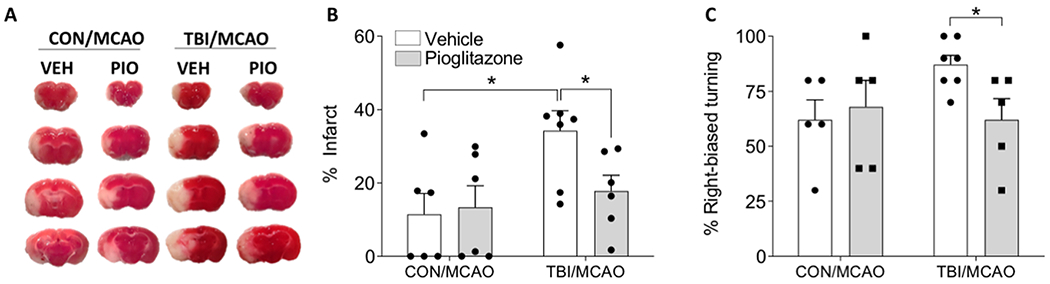
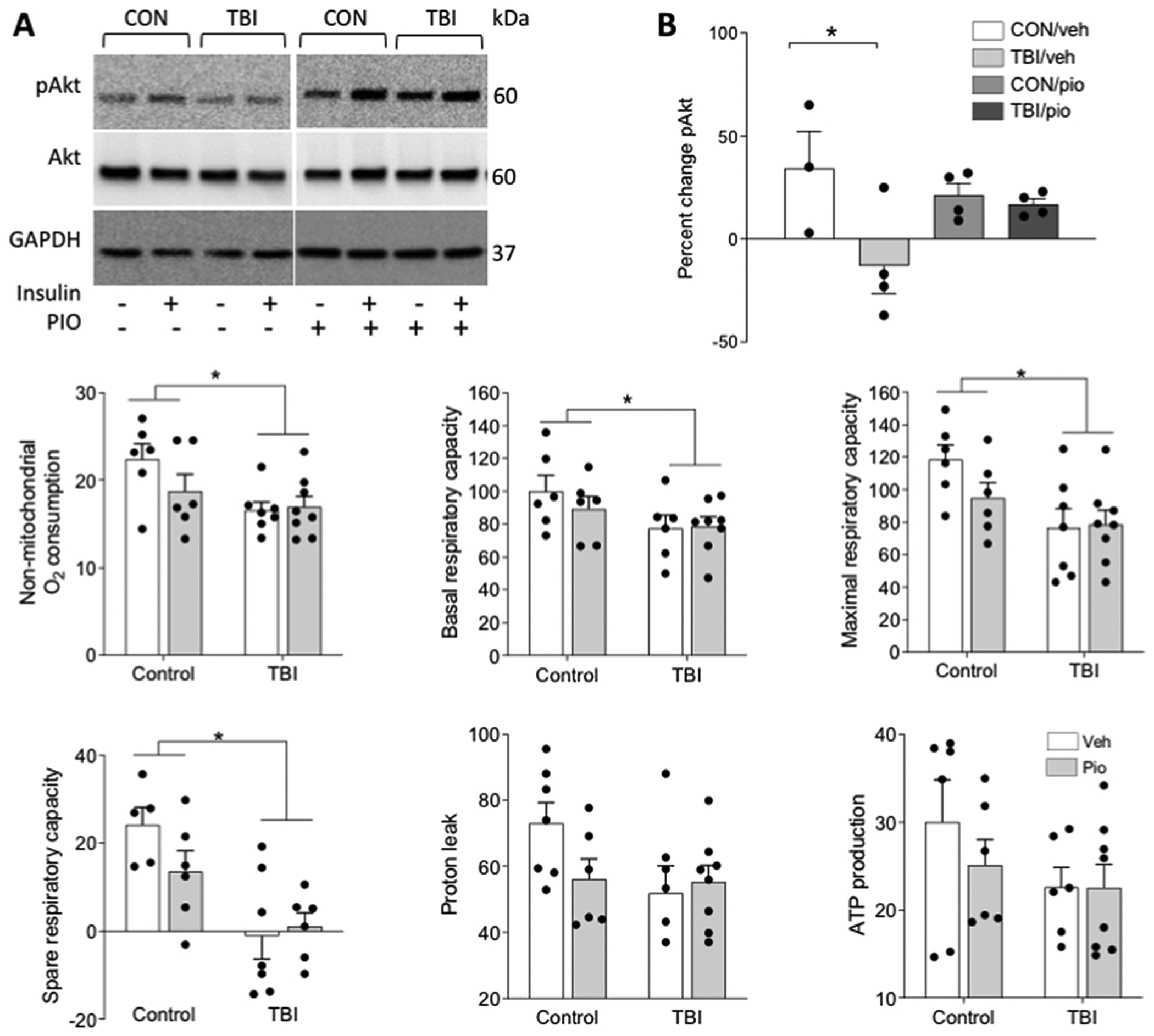
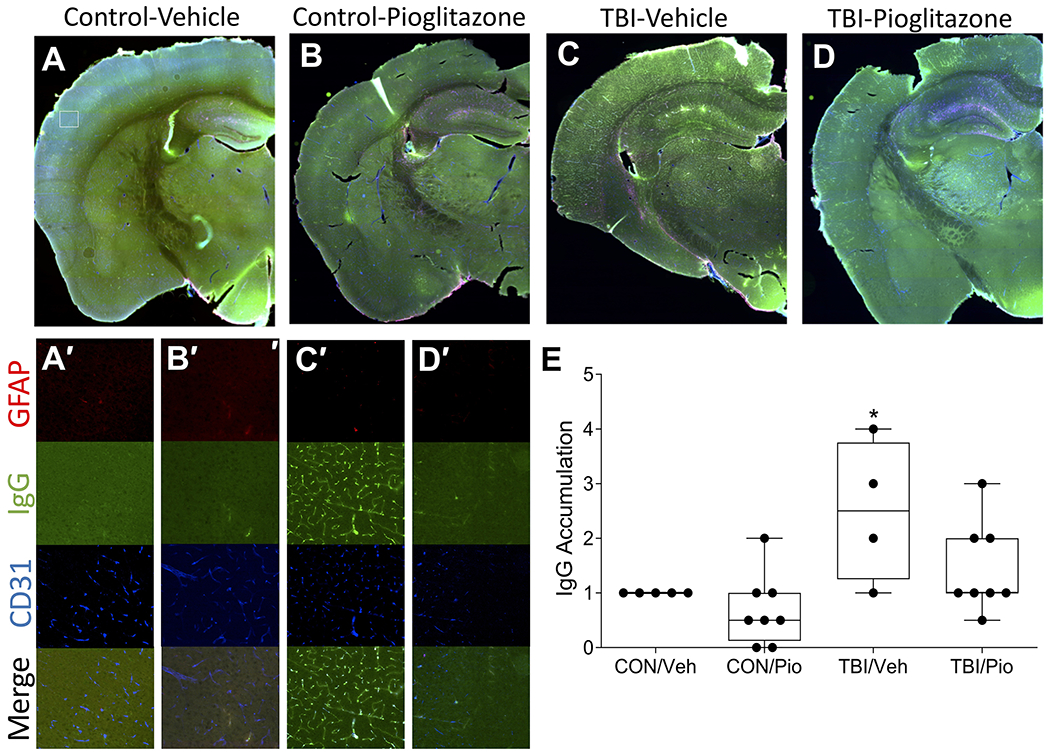
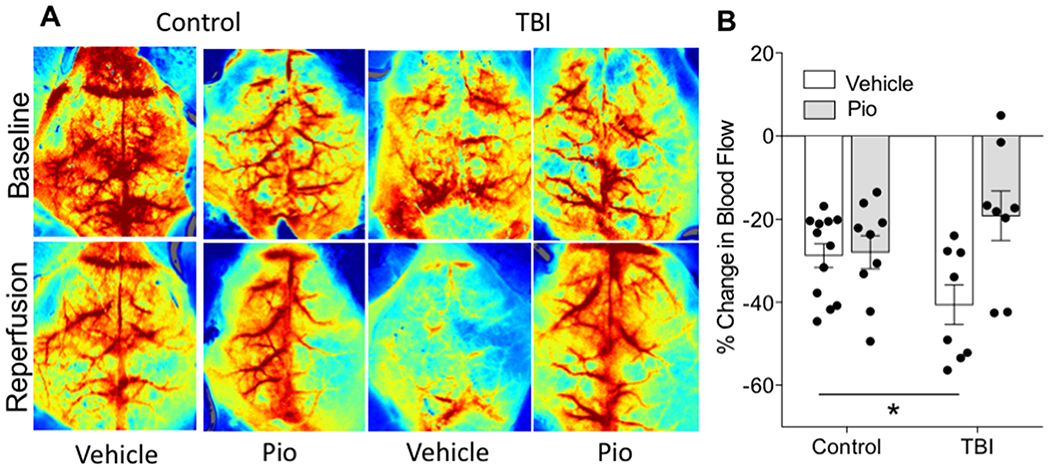
Recent studies have reported that TBI is an independent risk factor for subsequent stroke. Here, we tested the hypothesis that TBI would exacerbate experimental stroke outcomes via alternations in neuroimmune and neurometabolic function. We performed a mild closed-head TBI and then one week later induced an experimental stroke in adult male mice. Mice that had previously experienced TBI exhibited larger infarcts, greater functional deficits, and more pronounced neuroinflammatory responses to stroke. We hypothesized that impairments in central metabolic physiology mediated poorer outcomes after TBI. To test this, we treated mice with the insulin sensitizing drug pioglitazone (Pio) after TBI. Pio prevented the exacerbation of ischemic outcomes induced by TBI and also blocked the induction of insulin insensitivity by TBI. However, tissue respiratory function was not improved by Pio. Finally, TBI altered microvascular responses including promoting vascular accumulation of serum proteins and significantly impairing blood flow during the reperfusion period after stroke, both of which were reversed by treatment with Pio. Thus, TBI appears to exacerbate ischemic outcomes by impairing metabolic and microvascular physiology. These data have important implications because TBI patients experience strokes at greater rates than individuals without a history of head injury, but these data suggest that those strokes may also cause greater tissue damage and functional impairments in that population.
Keywords: Inflammation; Metabolism; Reperfusion; Stroke; Traumatic brain injury; Vasculature.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declarations of interest
None
Figures
References
-
- Abcouwer SF, Shanmugam S, Gomez PF, Shushanov S, Barber AJ, Lanoue KF, Quinn PG, Kester M, Gardner TW, 2008. Effect of IL-1beta on survival and energy metabolism of R28 and RGC-5 retinal neurons. Invest Ophthalmol Vis Sci 49, 5581–5592. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
