

Substituting Cannabidiol for Opioids and Pain Medications Among Individuals With Fibromyalgia: A Large Online Survey
- PMID: 33992787
- PMCID: PMC8578153
- DOI: 10.1016/j.jpain.2021.04.011
Substituting Cannabidiol for Opioids and Pain Medications Among Individuals With Fibromyalgia: A Large Online Survey
Abstract
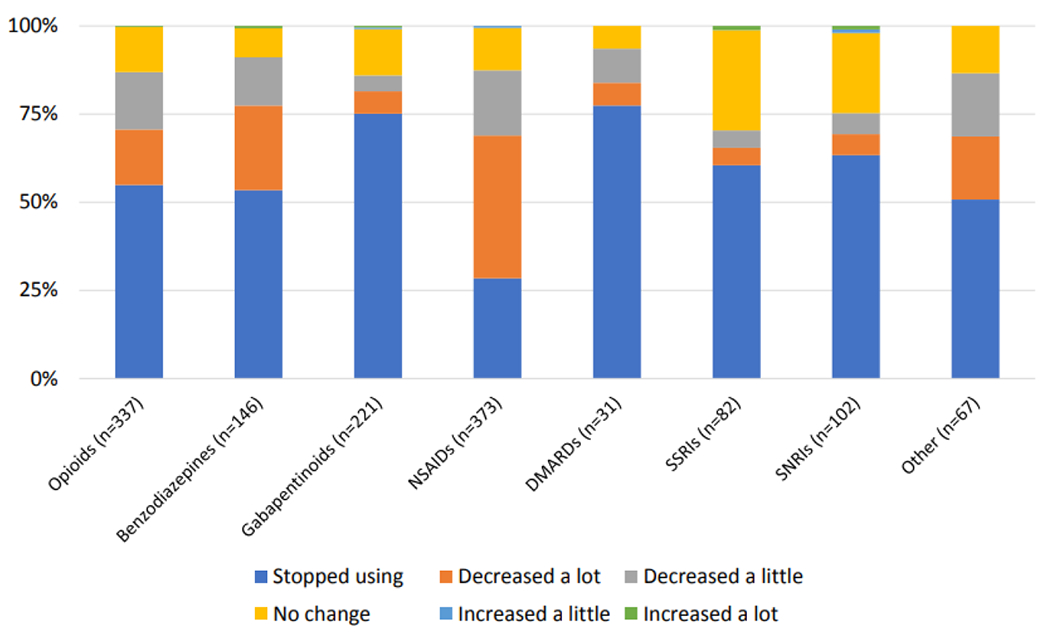
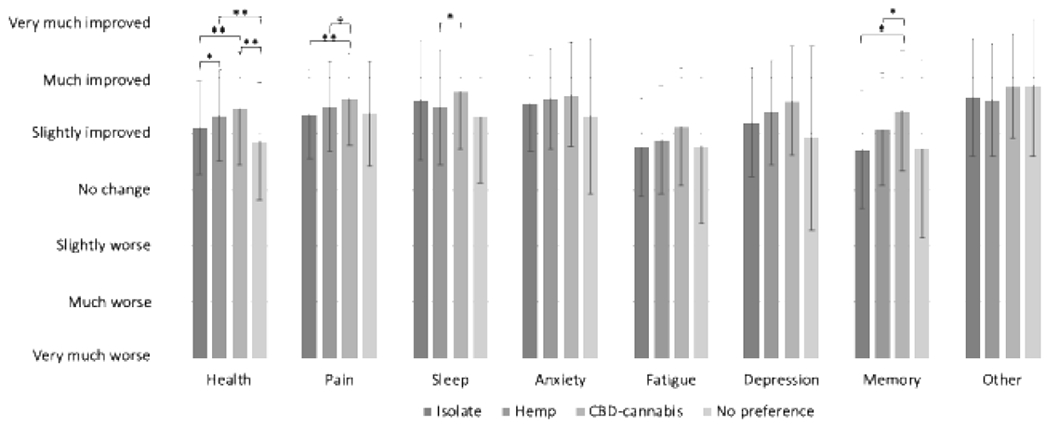
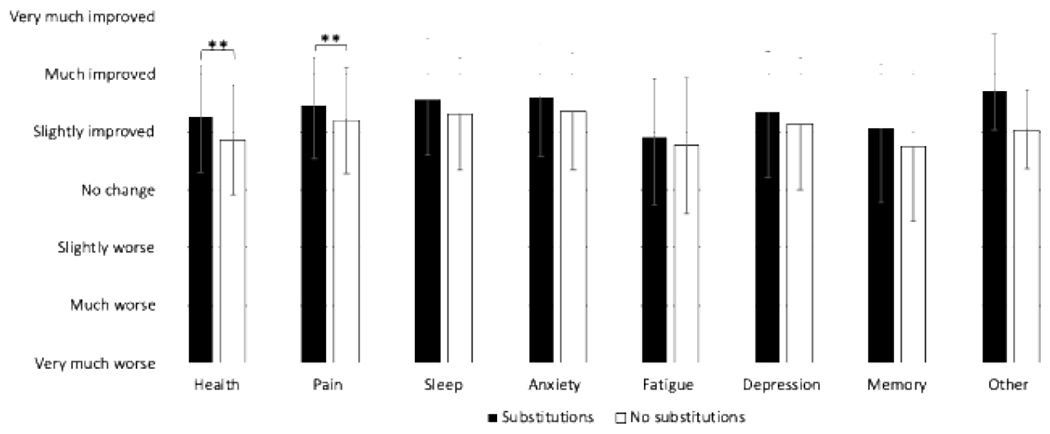
People report substituting cannabis for pain medications, but whether cannabidiol (CBD) is used similarly remains unknown. CBD products can be CBD alone (isolate), hemp extract (containing <0.3% Δ-9-tetrahydrocannabinol [THC], other cannabinoids, and terpenes), or CBD-cannabis (containing >0.3% THC). In a secondary analysis from a cross-sectional survey, we examined substitution patterns among n = 878 individuals with fibromyalgia who currently used CBD. We sub-grouped participants by most commonly used CBD product (CBD isolate, hemp, CBD-cannabis, no preference) and whether they substituted CBD for medications. We investigated rationale for substituting, substitution-driven medication changes, CBD use patterns, and changes in pain-related symptoms (eg, sleep, anxiety). The study population was 93.6% female and 91.5% Caucasian, with an average age of 55.5 years. The majority (n = 632, 72.0%) reported substituting CBD products for medications, most commonly NSAIDs (59.0%), opioids (53.3%), gabapentanoids (35.0%), and benzodiazepines (23.1%). Most substituting participants reported decreasing or stopping use of these pain medications. The most common reasons for substitution were fewer side effects and better symptom management. Age, hemp products, past-year use of marijuana, and higher somatic burden were all associated with substituting (P's ≤ .05). Those who substituted reported larger improvements in health and pain than those who did not. Participants using CBD-cannabis reported significantly more substitutions than any other group (P's ≤ .001) and larger improvements in health, pain, memory, and sleep than other subgroups. This widespread naturalistic substitution for pain medications suggests the need for more rigorous study designs to examine this effect. PERSPECTIVE: This article shows that people with fibromyalgia are deliberately substituting CBD products for conventional pain medications despite the dearth of evidence suggesting CBD products may be helpful for fibromyalgia. CBD's medication-sparing and therapeutic potential should be examined in more rigorous study designs.
Keywords: Cannabidiol; Fibromyalgia; Hemp; Opioids; Substitution.
Copyright © 2021 United States Association for the Study of Pain, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Cannabidiol Product Dosing and Decision-Making in a National Survey of Individuals with Fibromyalgia.J Pain. 2022 Jan;23(1):45-54. doi: 10.1016/j.jpain.2021.06.007. Epub 2021 Jun 30. J Pain. 2022. PMID: 34214700 Free PMC article.
-
Cannabidiol Use for Fibromyalgia: Prevalence of Use and Perceptions of Effectiveness in a Large Online Survey.J Pain. 2021 May;22(5):556-566. doi: 10.1016/j.jpain.2020.12.001. Epub 2021 Jan 2. J Pain. 2021. PMID: 33400996
-
Evaluation of the effects of CBD hemp extract on opioid use and quality of life indicators in chronic pain patients: a prospective cohort study.Postgrad Med. 2020 Jan;132(1):56-61. doi: 10.1080/00325481.2019.1685298. Epub 2019 Nov 12. Postgrad Med. 2020. PMID: 31711352 Clinical Trial.
-
Clinicians' Guide to Cannabidiol and Hemp Oils.Mayo Clin Proc. 2019 Sep;94(9):1840-1851. doi: 10.1016/j.mayocp.2019.01.003. Epub 2019 Aug 22. Mayo Clin Proc. 2019. PMID: 31447137 Review.
-
Can cannabidiol (CBD) help with low back pain?Ann Agric Environ Med. 2023 Sep 28;30(3):549-554. doi: 10.26444/aaem/168674. Epub 2023 Jul 12. Ann Agric Environ Med. 2023. PMID: 37772533 Review.
Cited by
-
Cannabidiol Product Dosing and Decision-Making in a National Survey of Individuals with Fibromyalgia.J Pain. 2022 Jan;23(1):45-54. doi: 10.1016/j.jpain.2021.06.007. Epub 2021 Jun 30. J Pain. 2022. PMID: 34214700 Free PMC article.
-
Thoughtfully Integrating Cannabis Products Into Chronic Pain Treatment.Anesth Analg. 2024 Jan 1;138(1):5-15. doi: 10.1213/ANE.0000000000005904. Epub 2023 Dec 15. Anesth Analg. 2024. PMID: 38100797 Free PMC article. Review.
-
Primary care provider attitudes, experiences and practices about cannabidiol (CBD) and barriers to patient-provider communication about CBD use: A qualitative study.PEC Innov. 2022 Apr 28;1:100044. doi: 10.1016/j.pecinn.2022.100044. eCollection 2022 Dec. PEC Innov. 2022. PMID: 37213726 Free PMC article.
-
Cannabidiol Perceptions and Use in the Orthopaedic Patient Population.JB JS Open Access. 2025 Apr 7;10(2):e24.00141. doi: 10.2106/JBJS.OA.24.00141. eCollection 2025 Apr-Jun. JB JS Open Access. 2025. PMID: 40196416 Free PMC article.
-
Genome-Wide Identification of NAC Family Genes and Their Expression Analyses in Response to Osmotic Stress in Cannabis sativa L.Int J Mol Sci. 2024 Aug 30;25(17):9466. doi: 10.3390/ijms25179466. Int J Mol Sci. 2024. PMID: 39273412 Free PMC article.
References
-
- Abuhasira R, Schleider LB, Mechoulam R, Novack V. Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly. Eur J Intern Med. 49:44–50, 2018 - PubMed
-
- Atwal N, Casey SL, Mitchell VA, Vaughan CW. THC and gabapentin interactions in a mouse neuropathic pain model. Neuropharmacology. 144:115–121, 2019 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
