

An examination of sedation requirements and practices for mechanically ventilated critically ill patients with COVID-19
- PMID: 33993212
- PMCID: PMC8194529
- DOI: 10.1093/ajhp/zxab202
An examination of sedation requirements and practices for mechanically ventilated critically ill patients with COVID-19
Abstract
Purpose: Preliminary reports suggest that critically ill patients with coronavirus disease 2019 (COVID-19) infection requiring mechanical ventilation may have markedly increased sedation needs compared with critically ill, mechanically ventilated patients without COVID-19. We conducted a study to examine sedative use for this patient population within multiple intensive care units (ICUs) of a large academic medical center.
Methods: A retrospective, single-center cohort study of sedation practices for critically ill patients with COVID-19 during the first 10 days of mechanical ventilation was conducted in 8 ICUs at Massachusetts General Hospital, Boston, MA. The study population was a sequential cohort of 86 critically ill, mechanically ventilated patients with COVID-19. Data characterizing the sedative medications, doses, drug combinations, and duration of administration were collected daily and compared to published recommendations for sedation of critically ill patients without COVID-19. The associations between drug doses, number of drugs administered, baseline patient characteristics, and inflammatory markers were investigated.
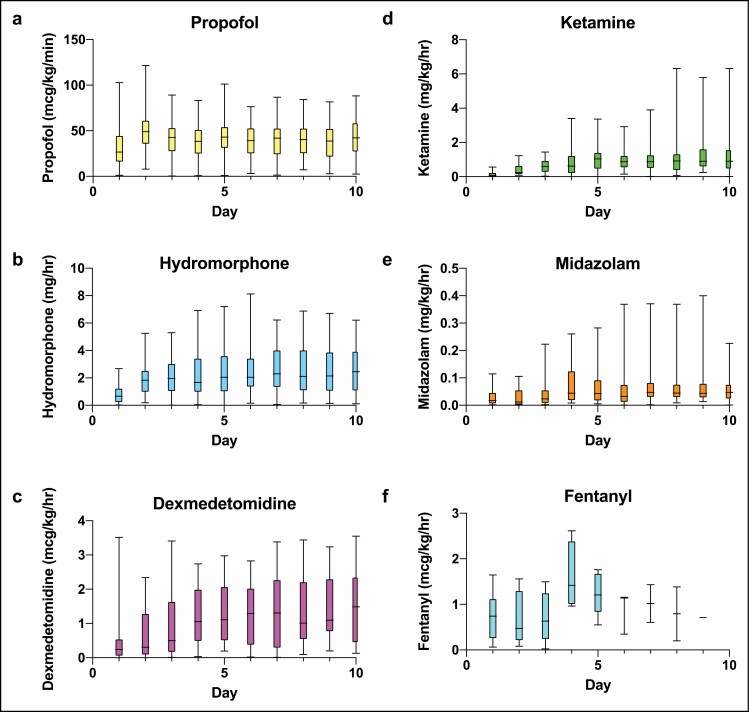
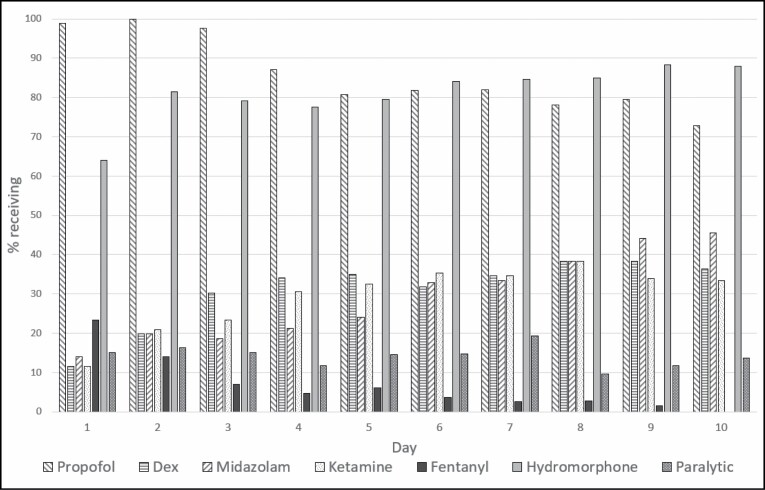
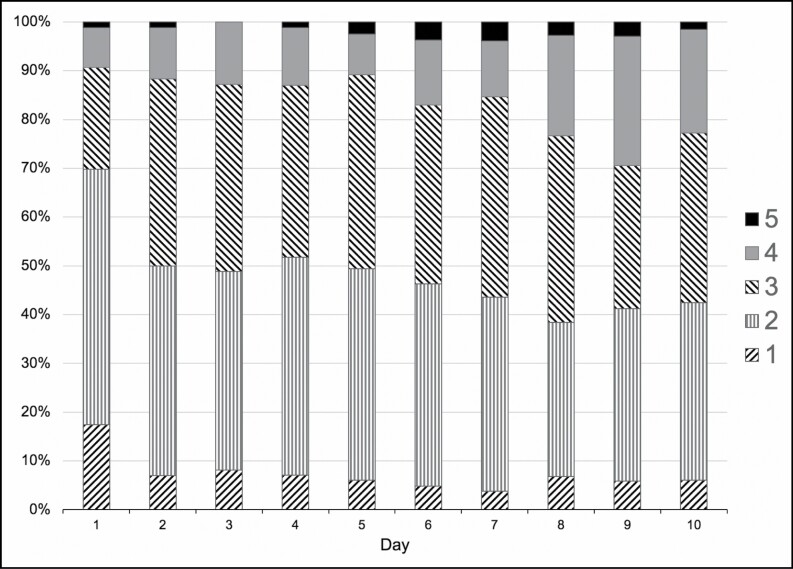
Results: Among the study cohort, propofol and hydromorphone were the most common initial drug combination, with these medications being used on a given day in up to 100% and 88% of patients, respectively. The doses of sedative and analgesic infusions increased for patients over the first 10 days, reaching or exceeding the upper limits of published dosage guidelines for propofol (48% of patients), dexmedetomidine (29%), midazolam (7.7%), ketamine (32%), and hydromorphone (38%). The number of sedative and analgesic agents simultaneously administered increased over time for each patient, with more than 50% of patients requiring 3 or more agents by day 2. Compared with patients requiring 3 or fewer agents, patients requiring more than 3 agents were of younger age, had an increased body mass index, had increased serum ferritin and lactate dehydrogenase concentrations, had a lower Pao2:Fio2 (ratio of arterial partial pressure of oxygen to fraction of inspired oxygen), and were more likely to receive neuromuscular blockade.
Conclusion: Our study confirmed the clinical impression of elevated sedative use in critically ill, mechanically ventilated patients with COVID-19 relative to guideline-recommended sedation practices in other critically ill populations.
Keywords: COVID-19; critical illness; mechanical ventilation; sedation.
© American Society of Health-System Pharmacists 2021. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- deBacker J, Hart N, Fan E. Neuromuscular blockade in the 21st century management of the critically ill patient. Chest. 2017;151:697-706. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
