

Prevention of Cardiac Dysfunction During Adjuvant Breast Cancer Therapy (PRADA): Extended Follow-Up of a 2×2 Factorial, Randomized, Placebo-Controlled, Double-Blind Clinical Trial of Candesartan and Metoprolol
- PMID: 33993702
- PMCID: PMC8212877
- DOI: 10.1161/CIRCULATIONAHA.121.054698
Prevention of Cardiac Dysfunction During Adjuvant Breast Cancer Therapy (PRADA): Extended Follow-Up of a 2×2 Factorial, Randomized, Placebo-Controlled, Double-Blind Clinical Trial of Candesartan and Metoprolol
Abstract
Background: Adjuvant breast cancer therapy containing anthracyclines with or without anti-human epidermal growth factor receptor-2 antibodies and radiotherapy is associated with cancer treatment-related cardiac dysfunction. In the PRADA trial (Prevention of Cardiac Dysfunction During Adjuvant Breast Cancer Therapy), concomitant treatment with the angiotensin receptor blocker candesartan attenuated the reduction in left ventricular ejection fraction (LVEF) in women receiving treatment for breast cancer, whereas the β-blocker metoprolol attenuated the increase in cardiac troponins. This study aimed to assess the long-term effects of candesartan and metoprolol or their combination to prevent a reduction in cardiac function and myocardial injury.
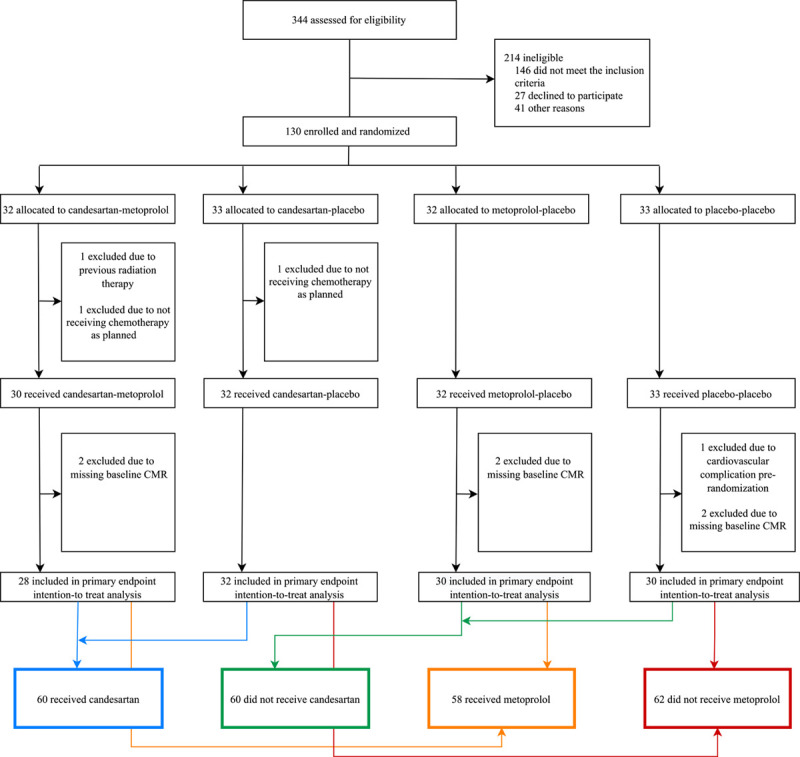
Methods: In this 2×2 factorial, randomized, placebo-controlled, double-blind, single-center trial, patients with early breast cancer were assigned to concomitant treatment with candesartan cilexetil, metoprolol succinate, or matching placebos. Target doses were 32 and 100 mg, respectively. Study drugs were discontinued after adjuvant therapy. All 120 validly randomized patients were included in the intention-to-treat analysis. The primary outcome measure was change in LVEF assessed by cardiovascular magnetic resonance imaging from baseline to extended follow-up. Secondary outcome measures included changes in left ventricular volumes, echocardiographic peak global longitudinal strain, and circulating cardiac troponin concentrations.
Results: A small decline in LVEF but no significant between-group differences were observed from baseline to extended follow-up, at a median of 23 months (interquartile range, 21 to 28 months) after randomization (candesartan, 1.7% [95% CI, 0.5 to 2.8]; no candesartan, 1.8% [95% CI, 0.6 to 3.0]; metoprolol, 1.6% [95% CI, 0.4 to 2.7]; no metoprolol, 1.9% [95% CI, 0.7 to 3.0]). Candesartan treatment during adjuvant therapy was associated with a significant reduction in left ventricular end-diastolic volume compared with the noncandesartan group (P=0.021) and attenuated decline in global longitudinal strain (P=0.046) at 2 years. No between-group differences in change in cardiac troponin I and T concentrations were observed.
Conclusions: Anthracycline-containing adjuvant therapy for early breast cancer was associated with a decline in LVEF during extended follow-up. Candesartan during adjuvant therapy did not prevent reduction in LVEF at 2 years, but was associated with modest reduction in left ventricular end-diastolic volume and preserved global longitudinal strain. These results suggest that a broadly administered cardioprotective approach may not be required in most patients with early breast cancer without preexisting cardiovascular disease. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT01434134.
Keywords: adrenergic beta-antagonists; angiotensin receptor antagonists; biomarkers; breast neoplasms; cardiomyopathies; magnetic resonance imaging.
Figures
References
-
- Strongman H, Gadd S, Matthews A, Mansfield KE, Stanway S, Lyon AR, Dos-Santos-Silva I, Smeeth L, Bhaskaran K. Medium and long-term risks of specific cardiovascular diseases in survivors of 20 adult cancers: a population-based cohort study using multiple linked UK electronic health records databases. Lancet. 2019;394:1041–1054. doi: 10.1016/S0140-6736(19)31674-5 - PMC - PubMed
-
- Zamorano JL, Lancellotti P, Rodriguez Muñoz D, Aboyans V, Asteggiano R, Galderisi M, Habib G, Lenihan DJ, Lip GYH, Lyon AR, et al. ; ESC Scientific Document Group. 2016 ESC position paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: the task force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J. 2016;37:2768–2801. doi: 10.1093/eurheartj/ehw211 - PubMed
-
- Jones LW, Haykowsky MJ, Swartz JJ, Douglas PS, Mackey JR. Early breast cancer therapy and cardiovascular injury. J Am Coll Cardiol. 2007;50:1435–1441. doi: 10.1016/j.jacc.2007.06.037 - PubMed
-
- Lenihan DJ, Fradley MG, Dent S, Brezden-Masley C, Carver J, Filho RK, Neilan TG, Blaes A, Melloni C, Herrmann J, et al. . Proceedings from the Global Cardio-Oncology Summit: the top 10 priorities to actualize for cardiooncology. JACC CardioOncol. 2019;1:256–272. doi: 10.1016/j.jaccao.2019.11.007 - PMC - PubMed
-
- Yusuf S, Pitt B, Davis CE, Hood WB, Cohn JN. SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med. 1991;325:293–302. doi: 10.1056/NEJM199108013250501 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
