

Fetal Goitrous Hyperthyroidism in a Pregnant Woman with Triiodothyronine-Predominant Graves' Disease
- PMID: 33994519
- PMCID: PMC8212807
Fetal Goitrous Hyperthyroidism in a Pregnant Woman with Triiodothyronine-Predominant Graves' Disease
Abstract
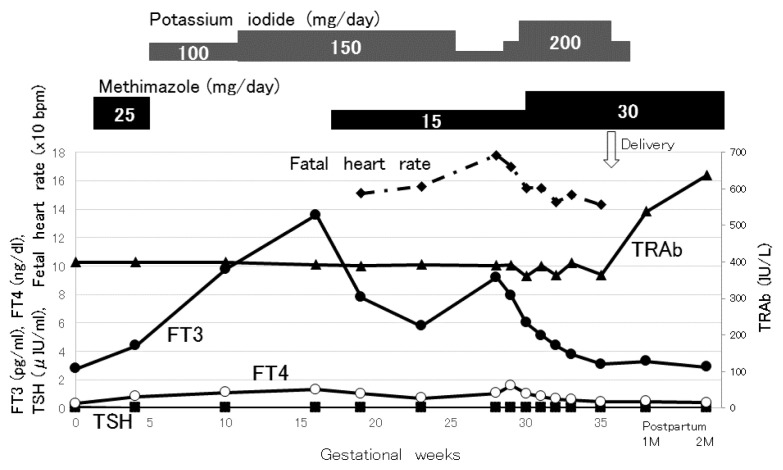
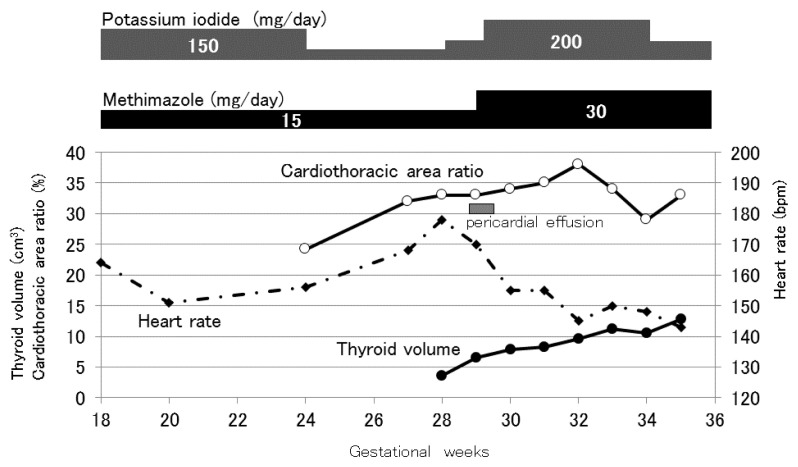
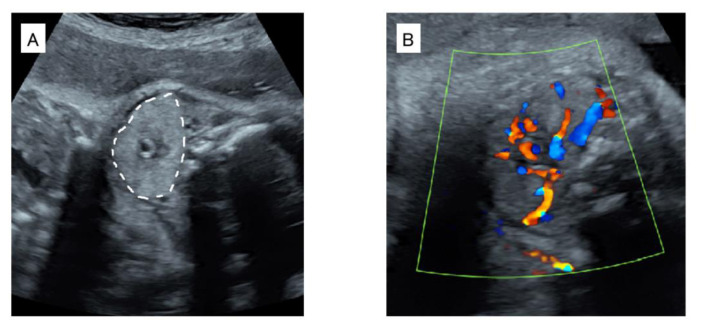
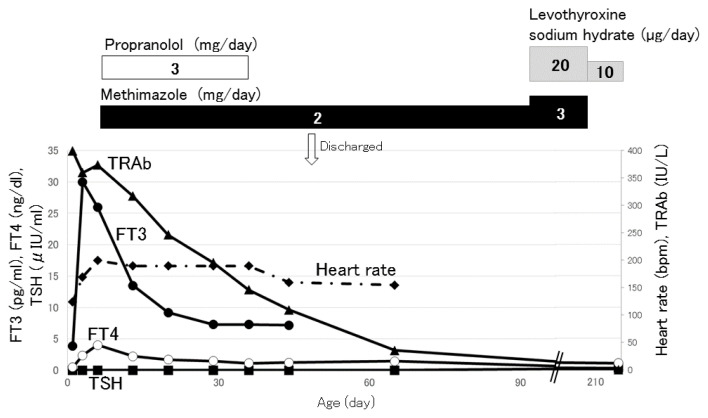
Triiodothyronine (T3)-predominant Graves' disease is characterized by increased serum free T3 (FT3) levels after free thyroxine (FT4) levels become normal or even low during antithyroid drug treatment. We encountered a 34-year-old pregnant woman, gravida 5 para 4, who was complicated by T3-predominant Graves' disease. She was diagnosed with Graves' disease at 20 years old, and had received methimazole. Methimazole was changed to potassium iodide to reduce the risk of congenital anomalies during the first trimester. The dose of antithyroid drugs was adjusted based on maternal FT4 levels, so that maternal Graves' disease deteriorated and fetal goitrous hyperthyroidism appeared during the second trimester. Since the fetus presented goiter and tachycardia at 27-28 gestational weeks, doses of methimazole and potassium iodide were increased. A male newborn weighing 2604 g was delivered by a cesarean section at 35 gestational weeks. The newborn was diagnosed with neonatal hyperthyroidism, and received methimazole for six months. He developed normally with normal thyroid function at 1 year old. In pregnancies complicated by T3-predominant Graves' disease, the kinds and doses of antithyroid drugs have to be carefully selected to maintain maternal levels of FT4 as well as FT3 within the normal range, considering trimesters of pregnancy, teratogenicity of medication, and maternal levels of thyroid-stimulating hormone receptor antibody.
Keywords: Graves' disease; antithyroid drug; fetal goiter; fetal hyperthyroidism; tachycardia.
Figures

References
-
- Andersen SL, Olsen J, Wu CS, Laurberg P. Birth defects after early pregnancy use of antithyroid drugs: a Danish nationawide study. J Clin Endocrinol Metab. 2013;98:4373–81. - PubMed
-
- Cooper DS, Rivkees SA. Putting propylthiouracil perspective. J Clin Endocrinol Metab. 2009;94:1881–2. - PubMed
-
- Corral E, Reascos M, Preiss Y, Rompel SM, Sepulveda W. Treatment of fetal goitrous hypothyroidism: value of direct intramuscular L-thyroxine therapy. Prenat Diagn. 2010;30:899–901. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources