

Long-term Outcomes with Carvedilol versus Propranolol in Patients with Index Variceal Bleed: 6-year Follow-up Study
- PMID: 33994717
- PMCID: PMC8103346
- DOI: 10.1016/j.jceh.2020.08.009
Long-term Outcomes with Carvedilol versus Propranolol in Patients with Index Variceal Bleed: 6-year Follow-up Study
Abstract
Aims and background: There is limited information on comparison of clinical outcomes with carvedilol for secondary prophylaxis following acute variceal bleed (AVB) when compared with propranolol. We report long-term clinical and safety outcomes of a randomised controlled trial comparing carvedilol with propranolol with respect to reduction in hepatic venous pressure gradient (HVPG) in patients after AVB.
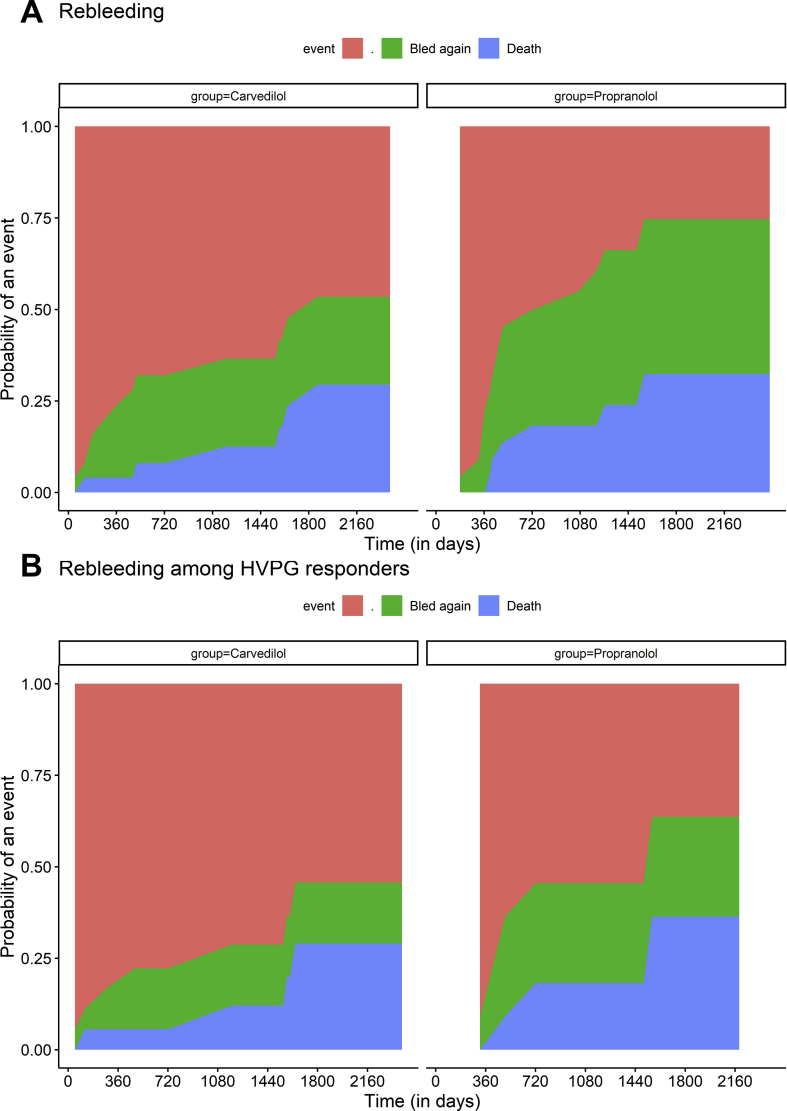
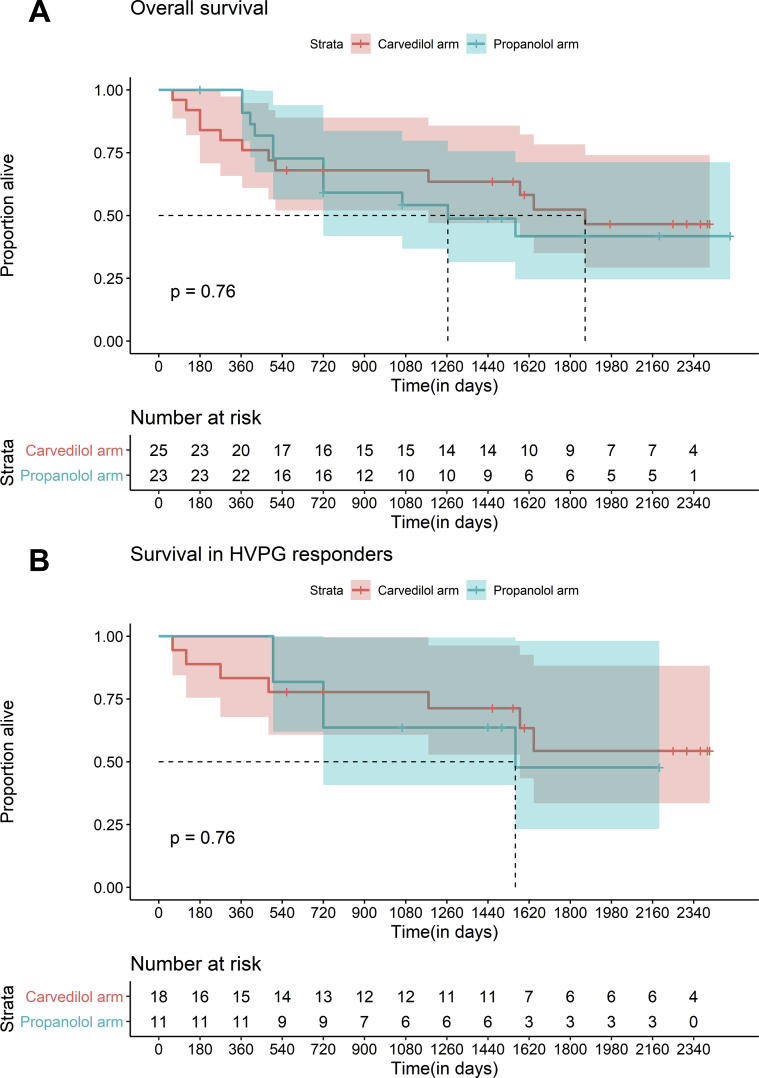
Methods: We conducted a post-hoc analysis of patients recruited in an open-label randomized controlled trial comparing carvedilol and propranolol following AVB, and estimated long-term rates of rebleed, survival, additional decompensation events and safety outcomes. Rebleed and other decompensations were compared using competing risks analysis, taking death as competing event, and survival was compared using Kaplan-Meier analysis.
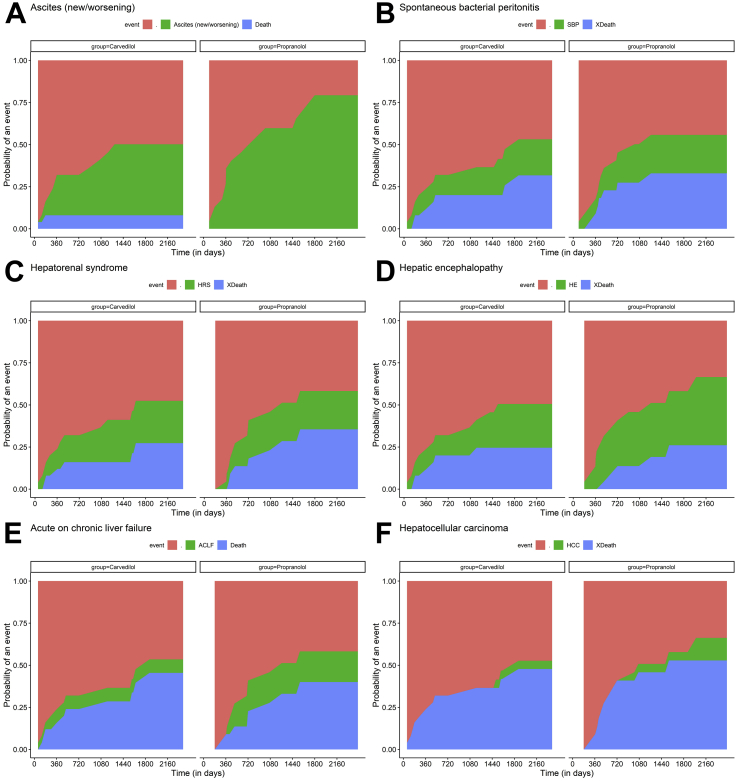
Results: Forty-eight patients (25 taking carvedilol; 23 propranolol) were followed up for 6 years from randomization. More number of patients on carvedilol had HVPG response when compared with those taking propranolol (72%- carvedilol versus 47.8% propranolol, p = 0.047). Comparable 1-year and 3-year rates of rebleed (16.0% and 24.0% for carvedilol versus 8.9% and 36.7% for propranolol; p = 0.457) and survival (94.7% and 89.0% for carvedilol versus 100.0% and 79.8% for propranolol; p = 0.76) were obtained. New/worsening ascites was more common in those receiving propranolol (69.5% vs 40%; p = 0.04). Other clinical decompensations and complications of liver disease occurred at comparable rates between two groups. Drug-related adverse-events were similar in both groups.
Conclusion: Despite higher degree of HVPG response, long-term clinical, survival and safety outcomes in carvedilol are similar to those of propranolol in patients with decompensated cirrhosis after index variceal bleed with the exception of ascites that developed less frequently in patients with carvedilol.
Keywords: ACLF, acute on chronic liver failure; AFP, alpha fetoprotein; AVB, acute variceal bleed; CT, computer tomography; CTP, Child–Turcotte–Pugh; EASL-CLIF, European Association of Study of Liver Disease-Chronic Liver Failure Consortium; EBL, endoscopic band ligation; HE, hepatic encephalopathy; HRS, hepatorenal syndrome; HVPG, hepatic venous portal gradient; MELD score; MELD, model for end-stage liver disease; NSBB, non-selective beta blockers; SBP, spontaneous bacterial peritonitis; UGIE, upper gastrointestinal endoscopy; acute variceal bleed; ascites; carvedilol; hepatic venous pressure gradient; propranolol; secondary prophylaxis.
© 2020 Indian National Association for Study of the Liver. Published by Elsevier B.V.
Figures
Similar articles
-
The Efficacy of Carvedilol in Comparison to Propranolol in Reducing the Hepatic Venous Pressure Gradient and Decreasing the Risk of Variceal Bleeding in Adult Cirrhotic Patients: A Systematic Review.Cureus. 2023 Aug 10;15(8):e43253. doi: 10.7759/cureus.43253. eCollection 2023 Aug. Cureus. 2023. PMID: 37577269 Free PMC article. Review.
-
Outcomes of Portal Pressure-Guided Therapy in Decompensated Cirrhosis With Index Variceal Bleed in Asian Cohort.J Clin Exp Hepatol. 2021 Jul-Aug;11(4):443-452. doi: 10.1016/j.jceh.2020.11.001. Epub 2020 Nov 13. J Clin Exp Hepatol. 2021. PMID: 34276151 Free PMC article.
-
Hemodynamic Response to Carvedilol is Maintained for Long Periods and Leads to Better Clinical Outcome in Cirrhosis: A Prospective Study.J Clin Exp Hepatol. 2016 Sep;6(3):175-185. doi: 10.1016/j.jceh.2016.01.004. Epub 2016 Jan 23. J Clin Exp Hepatol. 2016. PMID: 27746613 Free PMC article.
-
Combination of carvedilol with variceal band ligation in prevention of first variceal bleed in Child-Turcotte-Pugh B and C cirrhosis with high-risk oesophageal varices: the 'CAVARLY TRIAL'.Gut. 2024 Oct 7;73(11):1844-1853. doi: 10.1136/gutjnl-2023-331181. Gut. 2024. PMID: 39067870 Clinical Trial.
-
Carvedilol as the new non-selective beta-blocker of choice in patients with cirrhosis and portal hypertension.Liver Int. 2023 Jun;43(6):1183-1194. doi: 10.1111/liv.15559. Epub 2023 Apr 17. Liver Int. 2023. PMID: 36897563 Review.
Cited by
-
Acute-on-chronic liver failure is independently associated with higher mortality for cirrhotic patients with acute esophageal variceal hemorrhage: Retrospective cohort study.World J Clin Cases. 2023 Jun 16;11(17):4003-4018. doi: 10.12998/wjcc.v11.i17.4003. World J Clin Cases. 2023. PMID: 37388802 Free PMC article.
-
Long-Term Outcomes of Carvedilol Plus Endoscopic Variceal Ligation in Secondary Prophylaxis of Variceal Bleeding.Dig Dis Sci. 2025 Jun;70(6):2138-2146. doi: 10.1007/s10620-025-09000-3. Epub 2025 Apr 3. Dig Dis Sci. 2025. PMID: 40180690
-
The Efficacy of Carvedilol in Comparison to Propranolol in Reducing the Hepatic Venous Pressure Gradient and Decreasing the Risk of Variceal Bleeding in Adult Cirrhotic Patients: A Systematic Review.Cureus. 2023 Aug 10;15(8):e43253. doi: 10.7759/cureus.43253. eCollection 2023 Aug. Cureus. 2023. PMID: 37577269 Free PMC article. Review.
-
Development and Evaluation of a Physiologically Based Pharmacokinetic Drug-Disease Model of Propranolol for Suggesting Model Informed Dosing in Liver Cirrhosis Patients.Drug Des Devel Ther. 2021 Mar 17;15:1195-1211. doi: 10.2147/DDDT.S297981. eCollection 2021. Drug Des Devel Ther. 2021. PMID: 33762817 Free PMC article.
-
Overview of Complications in Cirrhosis.J Clin Exp Hepatol. 2022 Jul-Aug;12(4):1150-1174. doi: 10.1016/j.jceh.2022.04.021. Epub 2022 May 14. J Clin Exp Hepatol. 2022. PMID: 35814522 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
