

Delirium: A Marker of Vulnerability in Older People
- PMID: 33994990
- PMCID: PMC8119654
- DOI: 10.3389/fnagi.2021.626127
Delirium: A Marker of Vulnerability in Older People
Abstract
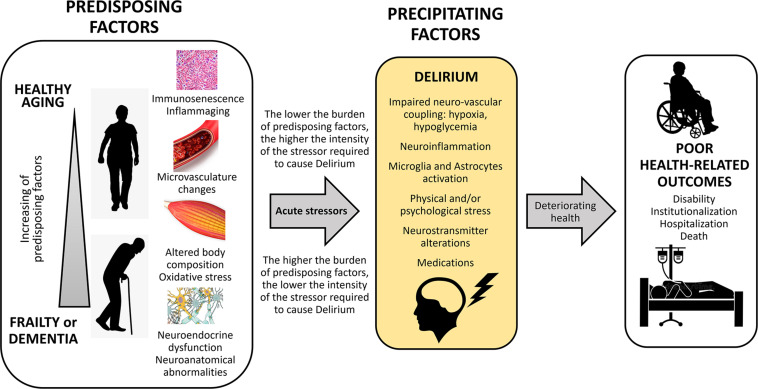
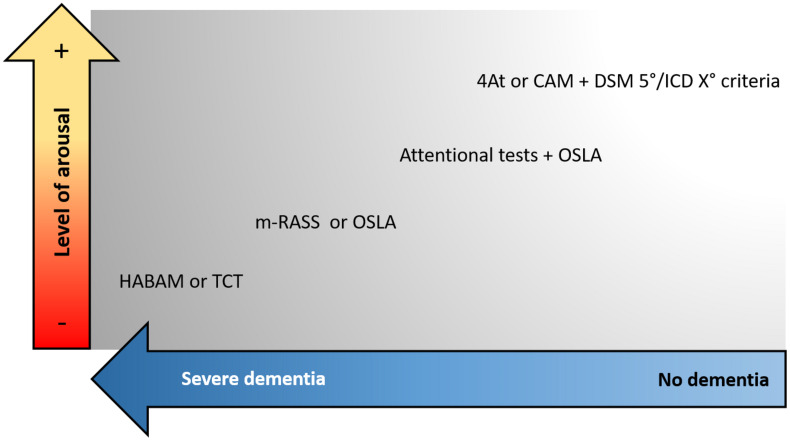
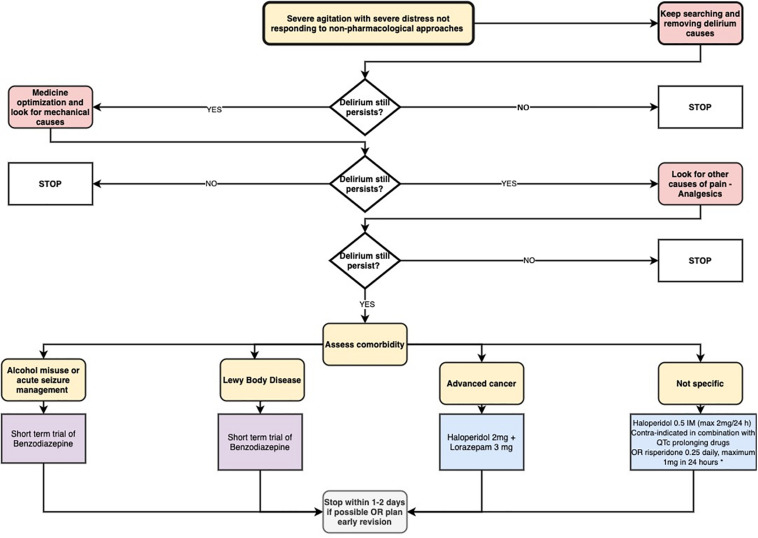
Delirium is an acute neuropsychiatric syndrome and one of the most common presenting symptoms of acute medical illnesses in older people. Delirium can be triggered by a single cause, but in most cases, it is multifactorial as it depends on the interaction between predisposing and precipitating factors. Delirium is highly prevalent in older patients across various settings of care and correlates with an increased risk of adverse clinical outcomes. Several pathophysiological mechanisms may contribute to its onset, including neurotransmitter imbalance, neuroinflammation, altered brain metabolism, and impaired neuronal network connectivity. Several screening and diagnostic tools for delirium exist, but they are unfortunately underutilized. Additionally, the diagnosis of delirium superimposed on dementia poses a formidable challenge - especially if dementia is severe. Non-pharmacological approaches for the prevention and multidomain interventions for the treatment of delirium are recommended, given that there is currently no robust evidence of drugs that can prevent or resolve delirium. This article aims to review the current understanding about delirium in older people. To achieve this goal, we will describe the epidemiology and outcomes of the syndrome, the pathophysiological mechanisms that are supposed to be involved, the most commonly used tools for screening and diagnosis, and prevention strategies and treatments recommended. This review is intended as a brief guide for clinicians in hospital wards to improve their knowledge and practice. At the end of the article, we propose an approach to improve the quality of care provided to older patients throughout a systematic detection of delirium.
Keywords: Atypical symptoms; confusion; delirium; elderly; frailty.
Copyright © 2021 Bellelli, Brathwaite and Mazzola.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: APA.
-
- Bellelli G., Frisoni G. B., Turco R., Lucchi E., Magnifico F., Trabucchi M. (2007). Delirium superimposed on dementia predicts 12-month survival in elderly patients discharged from a postacute rehabilitation facility. J. Gerontol. A Biol. Sci. Med. Sci. 62 1306–1309. 10.1093/gerona/62.11.1306 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical