

Fluid and White Matter Suppression Imaging and Voxel-Based Morphometric Analysis in Conventional Magnetic Resonance Imaging-Negative Epilepsy
- PMID: 33995250
- PMCID: PMC8116947
- DOI: 10.3389/fneur.2021.651592
Fluid and White Matter Suppression Imaging and Voxel-Based Morphometric Analysis in Conventional Magnetic Resonance Imaging-Negative Epilepsy
Abstract
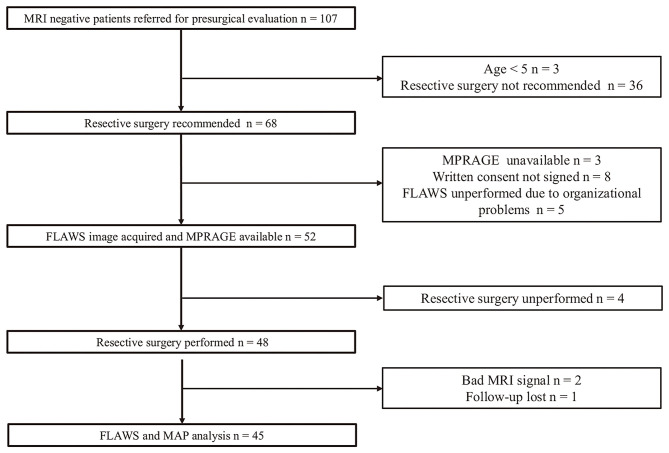
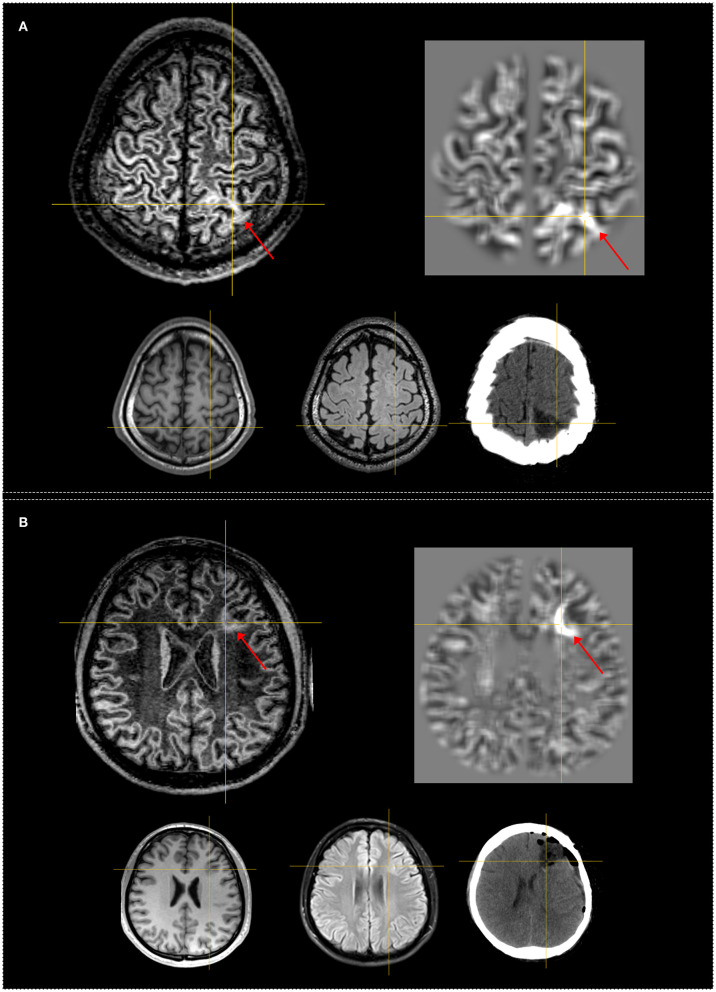
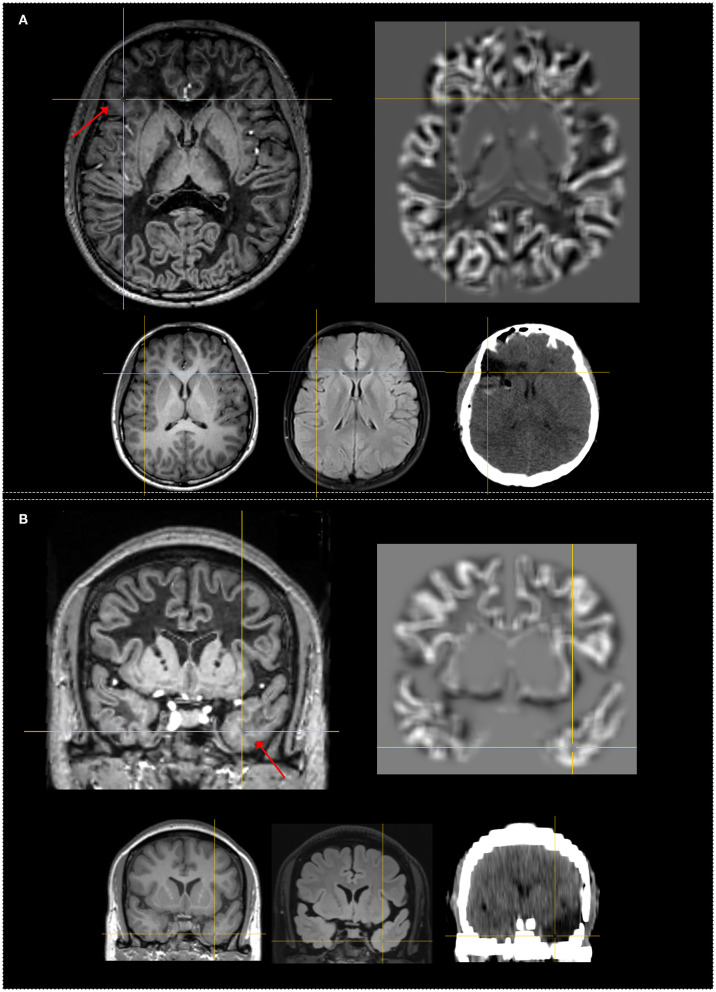
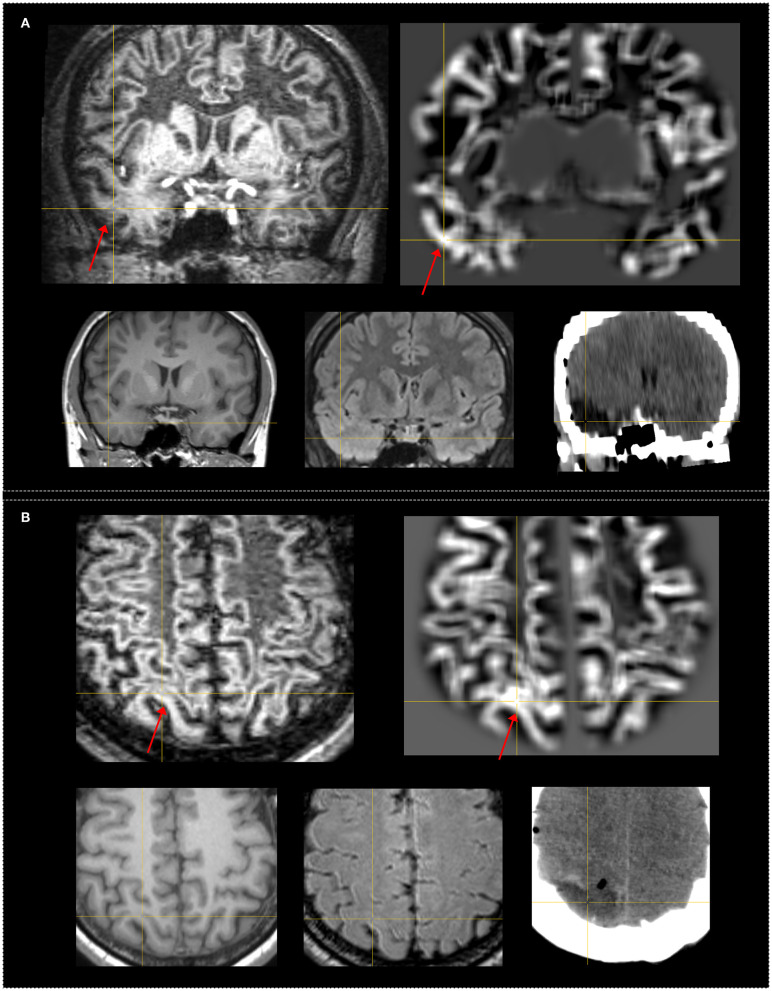
Purpose: Delineation of subtle lesions in magnetic resonance imaging (MRI)-negative patients is of great importance in preoperative epilepsy evaluation. The aim of our study was to explore the diagnostic value of the novel fluid and white matter suppression (FLAWS) sequence in comparison with a voxel-based MRI postprocessing morphometric analysis program (MAP) in a consecutive cohort of non-lesional patients. Methods: Surgical candidates with a negative finding on an official neuroradiology report were enrolled. High-resolution FLAWS image and MAP maps generated based on high-resolution three-dimensional (3D) T1 image were visually inspected for each patient. The findings of FLAWS or MAP-positive (FLAWS/MAP+) regions were compared with the surgical resection cavity in correlation with surgical outcome and pathology. Results: Forty-five patients were enrolled; the pathological examination revealed focal cortical dysplasia (FCD) in 32 patients and other findings in 13 patients. The positive rate, sensitivity, and specificity were 48.9%, 0.43, and 0.87, respectively, for FLAWS and 64.4%, 0.57, and 0.8, respectively, for MAP. Concordance between surgical resection and FLAWS+ or MAP+ regions was significantly associated with a seizure-free outcome (FLAWS: p = 0.002; MAP: p = 0.0003). A positive finding in FLAWS and MAP together with abnormalities in the same gyrus (FLAWS-MAP gyral+) was detected in 31.1% of patients. FLAWS+ only and MAP+ only were found in 7 (15.5%) and 14 (31.1%) patients, respectively. Conclusions: FLAWS showed a promising value for identifying subtle epileptogenic lesions and can be used as a complement to current MAP in patients with MRI-negative epilepsy.
Keywords: MRI post-processing; epilepsy; flaws; focal cortical dysplasia; non-lesional; voxel-based morphometric.
Copyright © 2021 Sun, Yu, Yang, Ren, Qiao, Ni, Wang, Zhao, Chen, Xiang, Chen, Gao, Yang, Lin, Kober and Zhang.
Conflict of interest statement
TK is a full employee of Siemens Healthcare AG Switzerland. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical