

Case Report: Complete Necrosis of a Large Adrenocortical Cancer and Liver Metastases Achieved by Selective Arterial Embolization: A Case Study and Review of Literature
- PMID: 33995288
- PMCID: PMC8121102
- DOI: 10.3389/fendo.2021.677187
Case Report: Complete Necrosis of a Large Adrenocortical Cancer and Liver Metastases Achieved by Selective Arterial Embolization: A Case Study and Review of Literature
Abstract
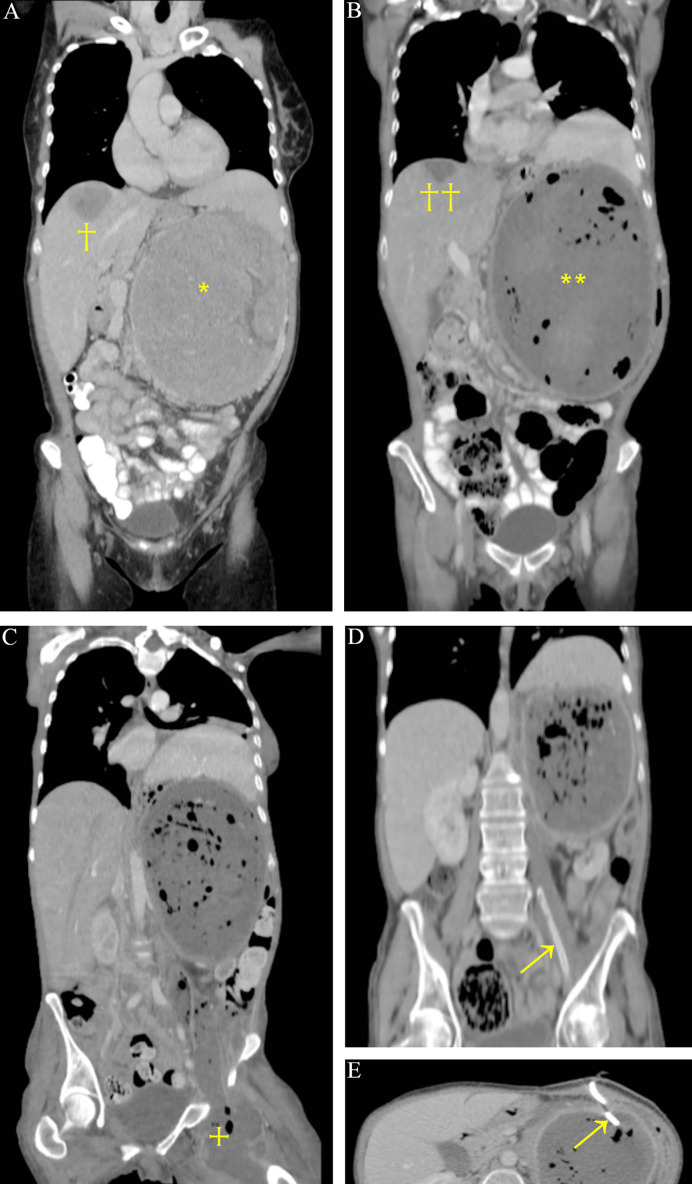
There is very limited experience regarding the interventional radiological treatment of adrenocortical cancer (ACC). We present the case of a 57-year-old female patient with a large, potentially unresectable left-sided ACC and two hepatic metastases. Both liver tumors were effectively treated by trans-arterial embolization (TAE), followed by TAE of the bulky primary tumor as a life-saving intervention necessitated by severe intratumoral bleeding. Surgical removal of the primary tumor revealed complete necrosis. The patient is considered tumor free after 3.5 years. To the best of our knowledge, this is the first report to show that even a primary ACC may be completely ablated by selective embolization, and the fourth to prove the curative potential of liver TAE for ACC metastases. This case highlights the potential of selective embolization in ACC treatment.
Keywords: adrenocortical cancer; embolization; liver metastasis; necrosis; trans-arterial.
Copyright © 2021 Huszty, Doros, Farkas, Kóbori, Reismann, Tőke, Tóth and Igaz.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Fassnacht M, Dekkers OM, Else T, Baudin E, Berruti A, de Krijger R, et al. . European Society of Endocrinology Clinical Practice Guidelines on the Management of Adrenocortical Carcinoma in Adults, in Collaboration With the European Network for the Study of Adrenal Tumors. Eur J Endocrinol (2018) 179:1–46. 10.1530/EJE-18-0608 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical