

Research Update on Stress Riser Fractures
- PMID: 33995860
- PMCID: PMC8081793
- DOI: 10.1007/s43465-020-00291-4
Research Update on Stress Riser Fractures
Abstract
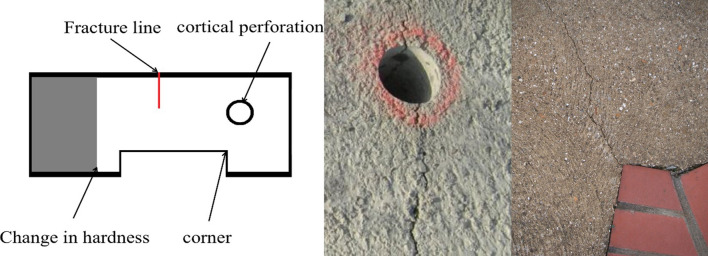
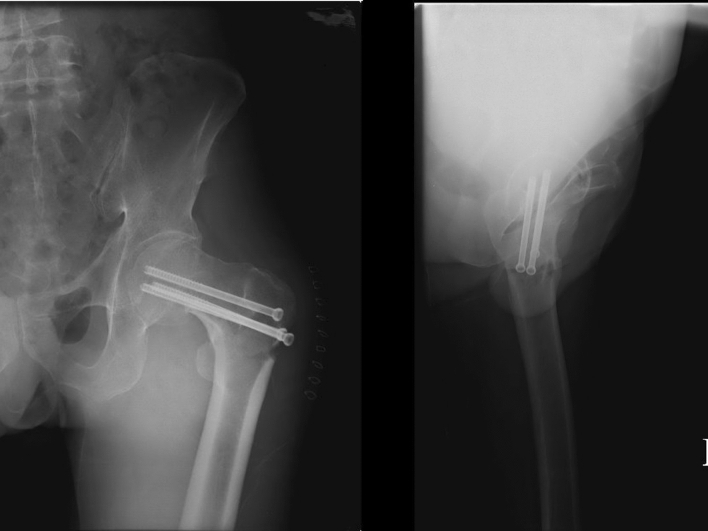
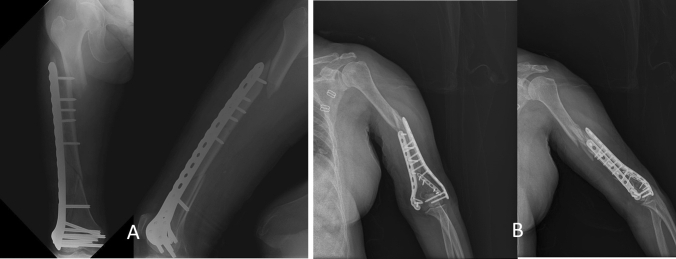
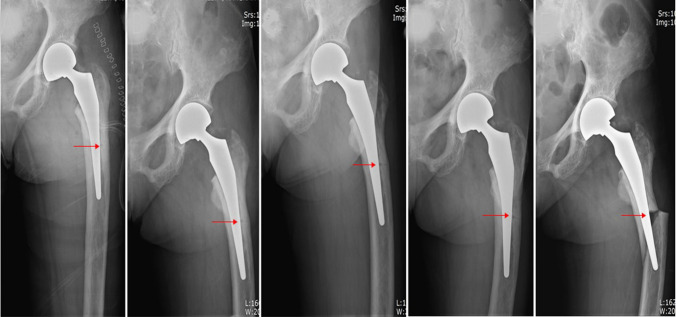
Stress fractures are fatigue-induced fractures which are caused by repetitive force, often from overuse. They are well-established and frequently encountered in the field of orthopedics. Stress fractures occur in the bone because of low-bone strength and high chronic mechanical stress placed on the bone. Stress riser fractures are also stress fractures that occur because of the presence of cortical defects (holes), changes in stiffness, sharp corners, and cracks (fracture lines). Periprosthetic or peri-implant fractures are good examples of stress riser fractures that occur in regions where stress forces are higher than those in the surrounding material. Most stress riser fractures are related to technical errors (iatrogenic causes) and are difficult to manage. It is possible and more effective to prevent the creation of stress riser fractures through better surgical techniques. The proper terminology for stress fractures, stress riser fractures, periprosthetic fractures, peri-implant fractures, interprosthetic fractures, and interimplant fractures is discussed. This review of the current state of knowledge, diagnosis, treatment, and prevention of stress riser fractures is based on clinical evidence and recent literature.
Keywords: Interimplant fracture; Interprosthetic fracture; Peri-implant fracture; Periprosthetic fracture; Stress fracture; Stress riser fracture.
© Indian Orthopaedics Association 2020.
Conflict of interest statement
Conflict of interestThe authors declare that they have no conflict of interest.
Figures
Similar articles
-
Mechanical analysis of femoral stress-riser fractures.Clin Biomech (Bristol). 2019 Mar;63:10-15. doi: 10.1016/j.clinbiomech.2019.02.004. Epub 2019 Feb 14. Clin Biomech (Bristol). 2019. PMID: 30784785
-
Minimally invasive double-plating osteosynthesis of the distal femur.Oper Orthop Traumatol. 2020 Dec;32(6):545-558. doi: 10.1007/s00064-020-00664-w. Epub 2020 Jun 16. Oper Orthop Traumatol. 2020. PMID: 32548732 English.
-
Small interprosthetic gaps do not increase femoral peri-prosthetic fracture risk. An in vitro biomechanical analysis.Acta Orthop Belg. 2017 Jun;83(2):197-204. Acta Orthop Belg. 2017. PMID: 30399982
-
Periprosthetic fractures about the knee - an overview.J Knee Surg. 2013 Feb;26(1):3-7. doi: 10.1055/s-0033-1333900. Epub 2013 Feb 7. J Knee Surg. 2013. PMID: 23393053 Review.
-
Periprosthetic fracture fixation in osteoporotic bone.Injury. 2016 Jun;47 Suppl 2:S44-50. doi: 10.1016/S0020-1383(16)47008-7. Injury. 2016. PMID: 27338227 Review.
Cited by
-
Peri-Implant Fracture After Distal Femur Percutaneous Epiphysiodesis Using Transphyseal Screws.J Pediatr Soc North Am. 2024 Feb 12;5(2):684. doi: 10.55275/JPOSNA-2023-684. eCollection 2023 May. J Pediatr Soc North Am. 2024. PMID: 40433516 Free PMC article.
-
[Off target of distal interlocking screw in short cephalomedullary nail fixation for intertrochanteric femur fractures].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 Mar 15;38(3):290-297. doi: 10.7507/1002-1892.202312001. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 38500421 Free PMC article. Chinese.
-
Periprosthetic Ulna Fractures Following Aptis Distal Radioulnar Joint Arthroplasty: A Series of Four Cases.J Hand Surg Glob Online. 2024 Aug 17;6(6):823-829. doi: 10.1016/j.jhsg.2024.06.012. eCollection 2024 Nov. J Hand Surg Glob Online. 2024. PMID: 39703600 Free PMC article.
-
Biomechanical evaluation of intramedullary retrograde nail and dynamic condylar screw used in unstable distal femoral fractures.Phys Eng Sci Med. 2023 Dec;46(4):1755-1764. doi: 10.1007/s13246-023-01335-3. Epub 2023 Oct 23. Phys Eng Sci Med. 2023. PMID: 37870727
-
Capitate Fracture Subsequent to Capitolunate Staple Fusion: A Case Report.J Hand Microsurg. 2024 Apr 16;16(1):100021. doi: 10.1055/s-0043-1761224. eCollection 2024 Mar. J Hand Microsurg. 2024. PMID: 38854383 Free PMC article.
References
-
- Laurence M, Freeman MAR, Swanson SAV. Engineering considerations in the internal fixation of fractures of the tibial shaft. The Journal of Bone and Joint Surgery. British Volume. 1969;51(4):754–768. - PubMed
-
- Cameron HU, Pilliar RM, Hastings DE, Fornasier VL. Iatrogenic subcapital fracture of the hip: A new complication of intertrochanteric fractures. Clinical Orthopaedics and Related Research. 1975;112:218–220. - PubMed
-
- Chan LWM, Gardner AW, Wong MK, Chua K, Kwek EBK. Non-prosthetic peri-implant fractures: Classification, management and outcomes. Archives of Orthopaedic and Trauma Surgery. 2018;138:791–802. - PubMed
Publication types
LinkOut - more resources
Full Text Sources