

Management of patients with BRCA mutation from the point of view of a breast surgeon
- PMID: 33996049
- PMCID: PMC8091883
- DOI: 10.1016/j.amsu.2021.102311
Management of patients with BRCA mutation from the point of view of a breast surgeon
Abstract
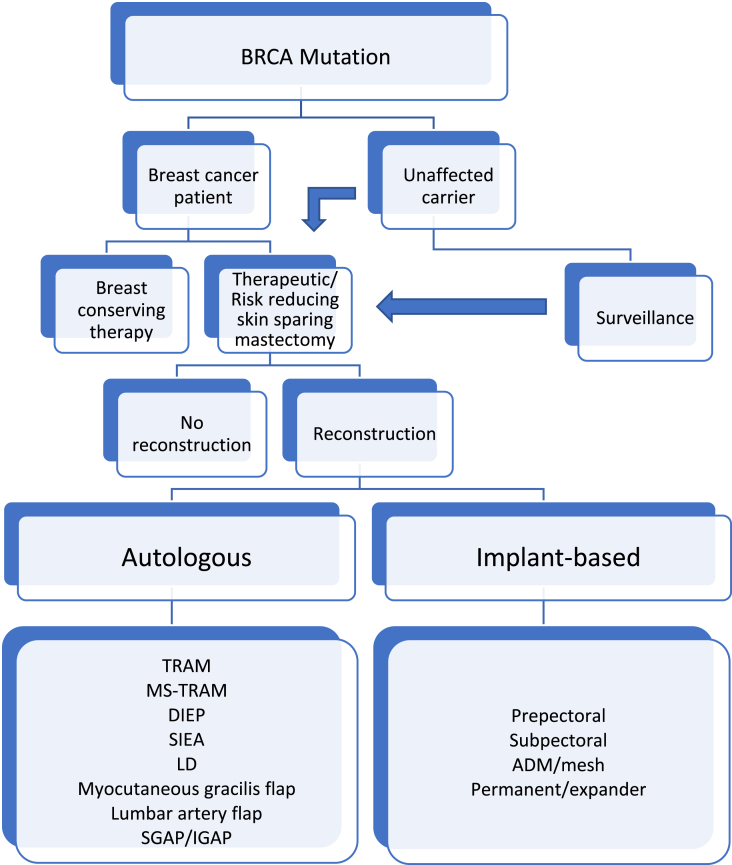
Germ-line mutation in BRCA (BReast CAncer gene) 1 or BRCA2 are found in 3-4% of all women with breast cancer. These patients have a significant increased risk of breast and ovarian cancer. They are often younger when diagnosed with the mutation, and the possible breast cancer they get is often aggressive with inferior outcome. There are risk reducing strategies, and the most powerful strategy is risk reducing surgery, both risk reducing bilateral mastectomy (RRM) and risk reducing bilateral salpino-oophorectomy (PBSO). This review is meant to address breast surgery in patients with germline BRCA mutation. The guidelines and techniques applied is under continuous change and it is important for the clinicians to be well informed to provide the patient with the information needed for them to make an informed decision on what risk strategy to choose.
Keywords: BRCA mutation; Breast cancer; Genetically caused breast cancer; Surgery.
© 2021 The Author.
Conflict of interest statement
The author confirms no conflict of interest.
Figures
Similar articles
-
Bilateral prophylactic mastectomy in BRCA mutation carriers: what surgeons need to know.Ann Ital Chir. 2019;90:1-2. Ann Ital Chir. 2019. PMID: 30872561
-
Risk-Reducing Bilateral Salpingo-Oophorectomy for BRCA Mutation Carriers and Hormonal Replacement Therapy: If It Should Rain, Better a Drizzle than a Storm.Medicina (Kaunas). 2019 Jul 29;55(8):415. doi: 10.3390/medicina55080415. Medicina (Kaunas). 2019. PMID: 31362334 Free PMC article.
-
Increased Overall Mortality Even after Risk Reducing Surgery for BRCA-Positive Women in Western Sweden.Genes (Basel). 2019 Dec 16;10(12):1046. doi: 10.3390/genes10121046. Genes (Basel). 2019. PMID: 31888263 Free PMC article.
-
Breast cancer treatment in mutation carriers: surgical treatment.Minerva Ginecol. 2016 Oct;68(5):548-56. Epub 2016 Jan 28. Minerva Ginecol. 2016. PMID: 26822896 Review.
-
The predominant role of surgery in the prevention and new trends in the surgical treatment of women with BRCA1/2 mutations.Ann Surg Oncol. 2008 Jan;15(1):21-33. doi: 10.1245/s10434-007-9612-4. Epub 2007 Oct 17. Ann Surg Oncol. 2008. PMID: 17940826 Review.
Cited by
-
Prophylactic Risk-Reducing Mastectomy (PRRM): A Set Practice or Catch-22 Situation in LMIC. A Single-Centre Prospective Cohort Study.World J Surg. 2023 Sep;47(9):2154-2160. doi: 10.1007/s00268-023-07033-1. Epub 2023 May 5. World J Surg. 2023. PMID: 37145137
-
Predictors of Recurrence and Overall Survival in Breast Cancer Patients Undergoing Neoadjuvant Chemotherapy and Surgery: A Comprehensive Statistical Analysis.Cancers (Basel). 2025 Mar 8;17(6):924. doi: 10.3390/cancers17060924. Cancers (Basel). 2025. PMID: 40149262 Free PMC article.
-
'Breast Cancer Resistance Likelihood and Personalized Treatment Through Integrated Multiomics'.Front Mol Biosci. 2022 Apr 14;9:783494. doi: 10.3389/fmolb.2022.783494. eCollection 2022. Front Mol Biosci. 2022. PMID: 35495618 Free PMC article. Review.
References
-
- Bray F., Ferlay J., Soerjomataram I., Siegel R.L., Torre L.A., Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018;68(6):394–424. - PubMed
-
- Hall J.M., Lee M.K., Newman B., Morrow J.E., Anderson L.A., Huey B. Linkage of early-onset familial breast cancer to chromosome 17q21. Science. 1990;250(4988):1684–1689. - PubMed
-
- Wooster R., Neuhausen S.L., Mangion J., Quirk Y., Ford D., Collins N. Localization of a breast cancer susceptibility gene, BRCA2, to chromosome 13q12-13. Science. 1994;265(5181):2088–2090. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
