

Evaluation and management of elbow injuries in the adolescent overhead athlete
- PMID: 33996078
- PMCID: PMC8072106
- DOI: 10.1177/20503121211003362
Evaluation and management of elbow injuries in the adolescent overhead athlete
Abstract
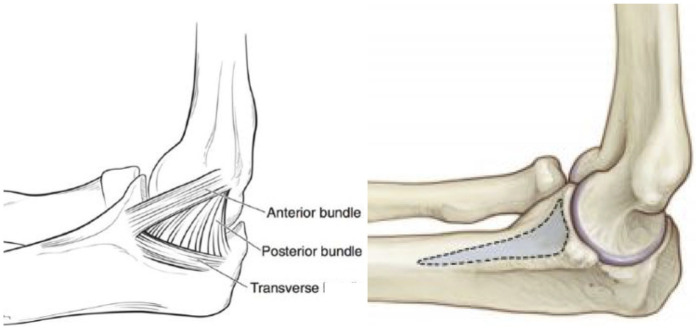
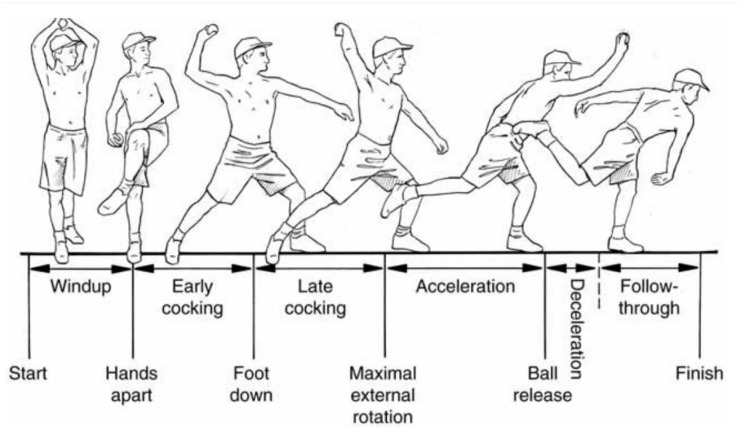
With an increased interest in youth sports, the burden of overhead throwing elbow injuries accompanying early single-sport focus has steadily risen. During the overhead throwing motion, valgus torque can reach and surpass Newton meters (N m) during the late cocking and early acceleration phases, which exceeds the tensile strength (22.7-33 N m) of the ulnar collateral ligament. While the ulnar collateral ligament serves as the primary valgus stabilizer between and degrees of elbow flexion, other structures about the elbow must contribute to stability during throwing. Depending on an athlete's stage of skeletal maturity, certain patterns of injury are observed with mechanical failures resulting from increased medial laxity, lateral-sided compression, and posterior extension shearing forces. Together, these injury patterns represent a wide range of conditions that arise from valgus extension overload. The purpose of this article is to review common pathologies observed in the adolescent overhead throwing athlete in the context of functional anatomy, osseous development, and throwing mechanics. Operative and non-operative management and their associated outcomes will be discussed for these injuries.
Keywords: Orthopedics; occupational therapy; rehabilitation.
© The Author(s) 2021.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Lawson BR, Comstock RD, Smith GA. Baseball-related injuries to children treated in hospital emergency departments in the United States, 1994–2006. Pediatrics 2009; 123(6): e1028–e1034. - PubMed
-
- Fleisig GS, Andrews JR, Cutter GR, et al. Risk of serious injury for young baseball pitchers: a 10-year prospective study. Am J Sports Med 2011; 39(2): 253–257. - PubMed
-
- Lansdown DA, Rugg CM, Feeley BT, et al. Single sport specialization in the skeletally immature athlete: current concepts. J Am Acad Orthop Surg 2020; 28: e752–e758. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
