Communicating personalized risks from COVID-19: guidelines from an empirical study
- PMID: 33996117
- PMCID: PMC8059635
- DOI: 10.1098/rsos.201721
Communicating personalized risks from COVID-19: guidelines from an empirical study
Abstract
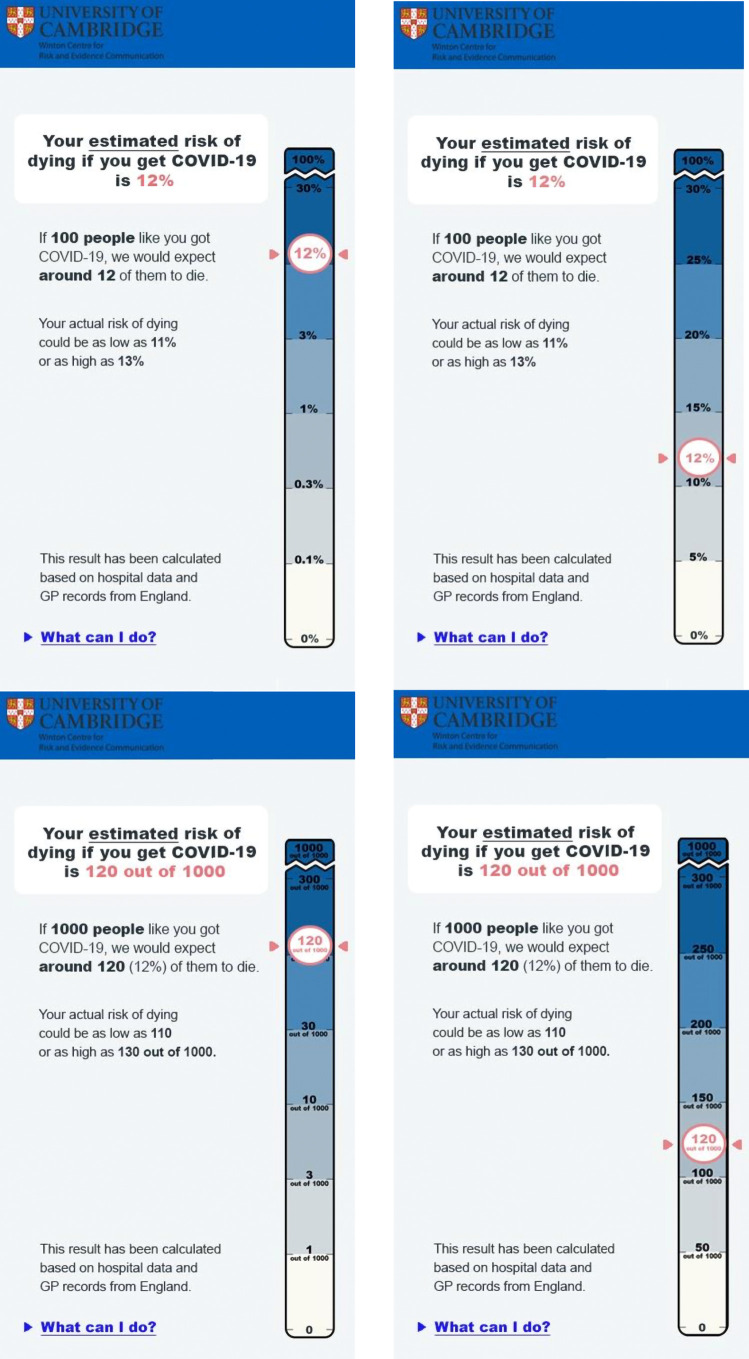
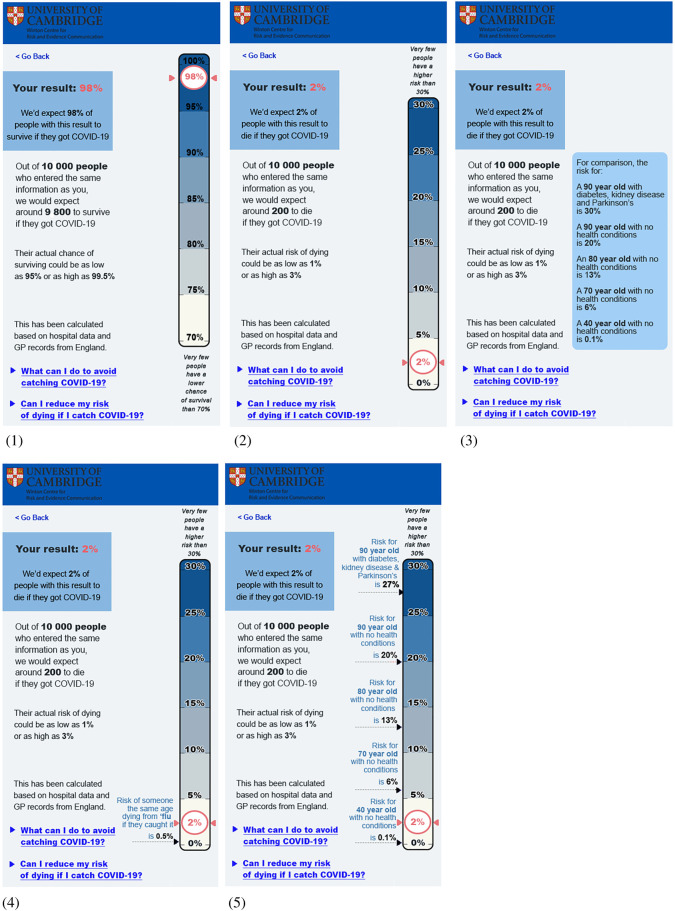
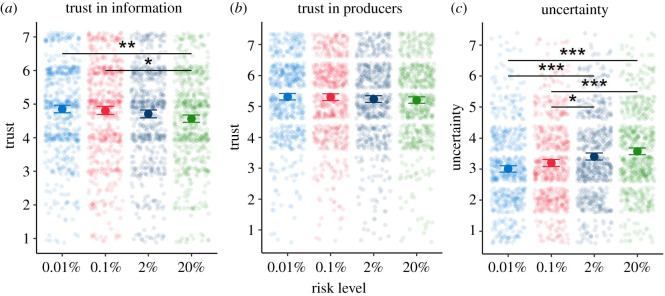
As increasing amounts of data accumulate on the effects of the novel coronavirus SARS-CoV-2 and the risk factors that lead to poor outcomes, it is possible to produce personalized estimates of the risks faced by groups of people with different characteristics. The challenge of how to communicate these then becomes apparent. Based on empirical work (total n = 5520, UK) supported by in-person interviews with the public and physicians, we make recommendations on the presentation of such information. These include: using predominantly percentages when communicating the absolute risk, but also providing, for balance, a format which conveys a contrasting (higher) perception of risk (expected frequency out of 10 000); using a visual linear scale cut at an appropriate point to illustrate the maximum risk, explained through an illustrative 'persona' who might face that highest level of risk; and providing context to the absolute risk through presenting a range of other 'personas' illustrating people who would face risks of a wide range of different levels. These 'personas' should have their major risk factors (age, existing health conditions) described. By contrast, giving people absolute likelihoods of other risks they face in an attempt to add context was considered less helpful. We note that observed effect sizes generally were small. However, even small effects are meaningful and relevant when scaled up to population levels.
Keywords: COVID-19; risk communication; risk perception.
© 2021 The Authors.
Figures

















References
-
- Slovic P, Fischoff B, Lichtenstein S. 1981. Perceived risk: psychological factors and social implications. Proc. R. Soc. Lond. A 376, 17-34. (10.1098/rspa.1981.0073) - DOI
-
- Fischhoff B, Slovic P, Lichtenstein S, Read S, Combs B. 1978. How safe is safe enough? A psychometric study of attitudes towards technological risks and benefits. Policy Sci. 9, 127-152. (10.1007/BF00143739) - DOI
-
- Dryhurst S, Schneider CR, Kerr J, Freeman ALJ, Recchia G, van der Bles AM, Spiegelhalter D, van der Linden S. 2020. Risk perceptions of COVID-19 around the world. J. Risk Res. 23, 1466-4461. (10.1080/13669877.2020.1758193) - DOI
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous