

Accuracy of homogeneous models for photon diffusion in estimating neonatal cerebral hemodynamics by TD-NIRS
- PMID: 33996206
- PMCID: PMC8086468
- DOI: 10.1364/BOE.417357
Accuracy of homogeneous models for photon diffusion in estimating neonatal cerebral hemodynamics by TD-NIRS
Abstract
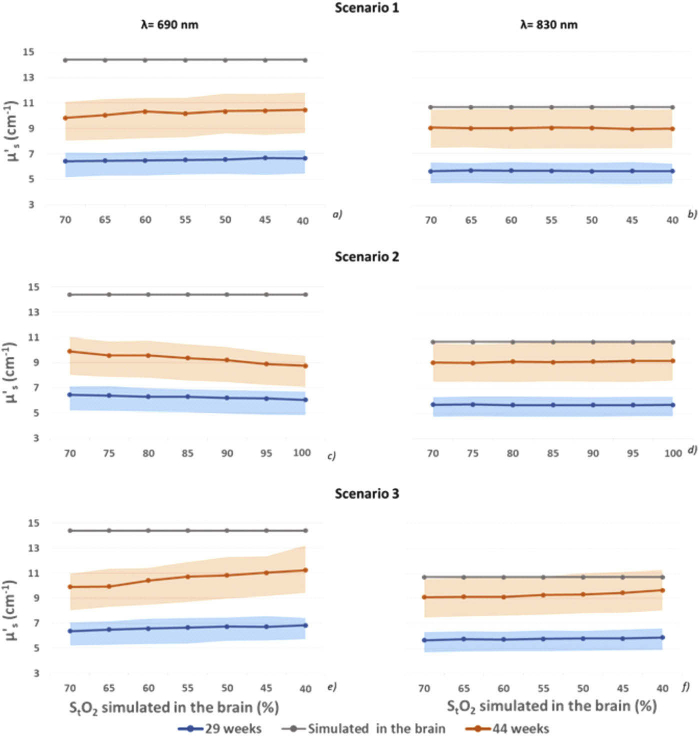
We assessed the accuracy of homogenous (semi-infinite, spherical) photon diffusion models in estimating absolute hemodynamic parameters of the neonatal brain in realistic scenarios (ischemia, hyperoxygenation, and hypoventilation) from 1.5 cm interfiber distance TD NIRS measurements. Time-point-spread-functions in 29- and 44-weeks postmenstrual age head meshes were simulated by the Monte Carlo method, convoluted with a real instrument response function, and then fitted with photon diffusion models. The results show good accuracy in retrieving brain oxygen saturation, and severe underestimation of total cerebral hemoglobin, suggesting the need for more complex models of analysis or of larger interfiber distances to precisely monitor all hemodynamic parameters.
© 2021 Optical Society of America under the terms of the OSA Open Access Publishing Agreement.
Conflict of interest statement
The authors declare that there are no conflicts of interest related to this article.
Figures






References
LinkOut - more resources
Full Text Sources
Other Literature Sources