

Perspectives on urological care in multiple sclerosis patients
- PMID: 33996350
- PMCID: PMC8122310
- DOI: 10.5582/irdr.2021.01029
Perspectives on urological care in multiple sclerosis patients
Abstract
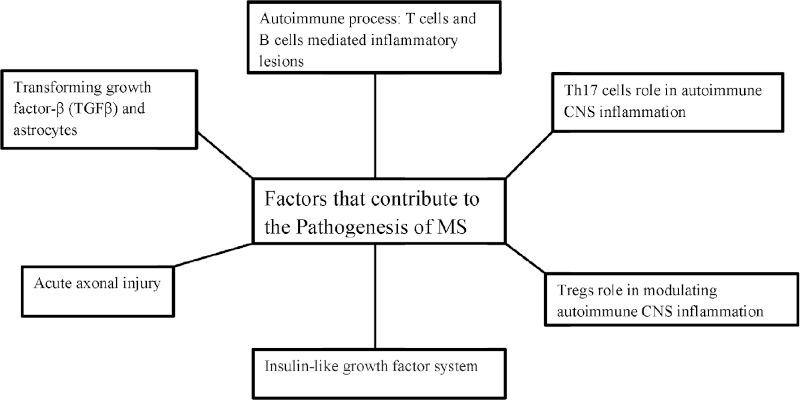
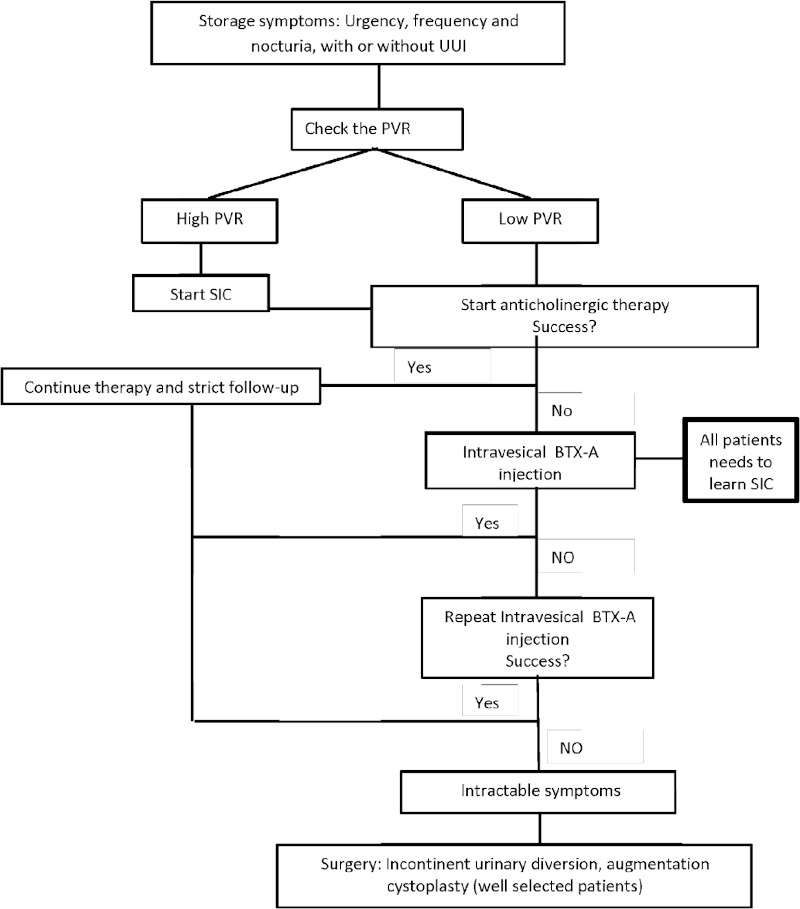
Multiple sclerosis (MS) is a chronic autoimmune disease of the central nervous system. Lower urinary tract dysfunction due to MS includes a dysfunction of the storage phase or dysfunction of the voiding phase or a detrusor-sphincter dyssynergia. Baseline evaluation includes a voiding chart, an ultrasound scan of the urinary tract, urine culture, and an urodynamic study. For storage symptoms, antimuscarinics are the first-line treatment, and clean intermittent catheterization (CIC) is indicated if there is concomitant incomplete bladder emptying. Intradetrusor injections with botulinum toxin A (BTX-A), are recommended for refractory cases. Urinary diversion is rarely indicated. For patients with voiding symptoms, CIC and alpha-blockers are usually offered. Sexual dysfunction in patients with MS is multifactorial. Phosphodiesterase type 5 inhibitors are first-line therapies for MS-associated erectile dysfunction in both male and female patients. This review summarizes the epidemiology, pathogenesis, risk factors, genetic, clinical manifestations, diagnostic tests, and management of MS. Lastly, the urologic outcomes and therapies are reviewed.
Keywords: lower urinary tract dysfunction; multiple sclerosis; neurogenic bladder; urology.
2021, International Research and Cooperation Association for Bio & Socio - Sciences Advancement.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Single-institution experience in 110 patients with botulinum toxin A injection into bladder or urethra.Urology. 2005 Jan;65(1):37-41. doi: 10.1016/j.urology.2004.08.016. Urology. 2005. PMID: 15667859
-
Lower urinary tract dysfunction in patients with multiple sclerosis.Handb Clin Neurol. 2015;130:371-81. doi: 10.1016/B978-0-444-63247-0.00021-3. Handb Clin Neurol. 2015. PMID: 26003255 Review.
-
Nocturia in Patients With Multiple Sclerosis.Rev Urol. 2019;21(2-3):63-73. Rev Urol. 2019. PMID: 31768133 Free PMC article.
-
Botulinum toxin as a new therapy option for voiding disorders: current state of the art.Eur Urol. 2003 Aug;44(2):165-74. doi: 10.1016/s0302-2838(03)00250-1. Eur Urol. 2003. PMID: 12875934 Review.
-
The use of botulinum toxin A injection for the management of external sphincter dyssynergia in neurologically normal children.J Urol. 2007 Oct;178(4 Pt 2):1775-9; discussion 1779-80. doi: 10.1016/j.juro.2007.03.185. Epub 2007 Aug 17. J Urol. 2007. PMID: 17707430
Cited by
-
Case report: Case series of urinary retention in young adults with severe autism hospitalized for behavioral crisis.Front Psychiatry. 2025 May 13;16:1570436. doi: 10.3389/fpsyt.2025.1570436. eCollection 2025. Front Psychiatry. 2025. PMID: 40433175 Free PMC article.
-
The Effect of Bio-Electromagnetic Energy Regulation Therapy on Erectile Dysfunction in Patients with Multiple Sclerosis: A Triple-Blind Randomized Clinical Trial.J Clin Med. 2024 Nov 22;13(23):7060. doi: 10.3390/jcm13237060. J Clin Med. 2024. PMID: 39685520 Free PMC article.
-
Voiding Phase Dysfunction in Multiple Sclerosis: Contemporary Review of Terminology, Diagnosis, Management, and Future Directions.Urol Clin North Am. 2024 May;51(2):177-185. doi: 10.1016/j.ucl.2024.01.005. Epub 2024 Mar 4. Urol Clin North Am. 2024. PMID: 38609190 Free PMC article. Review.
References
-
- Dobson R, Giovannoni G. Multiple sclerosis - a review. Eur J Neurol. 2019; 26:27-40. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous