

Radiation-Induced Soft Tissue Injuries in Patients With Advanced Mandibular Osteoradionecrosis: A Preliminary Evaluation and Management of Various Soft Tissue Problems Around Radiation-Induced Osteonecrosis Lesions
- PMID: 33996554
- PMCID: PMC8113699
- DOI: 10.3389/fonc.2021.641061
Radiation-Induced Soft Tissue Injuries in Patients With Advanced Mandibular Osteoradionecrosis: A Preliminary Evaluation and Management of Various Soft Tissue Problems Around Radiation-Induced Osteonecrosis Lesions
Abstract
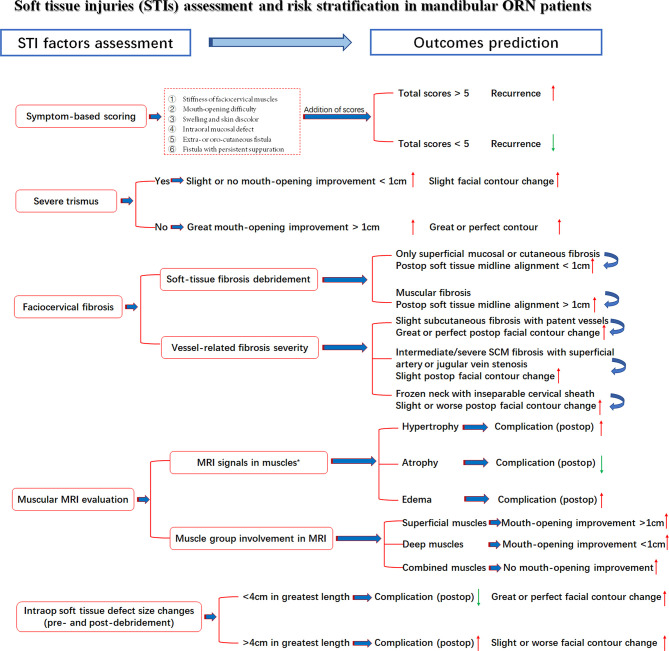
Objectives: Radiation-induced soft-tissue injuries (STIs) in mandibular osteoradionecrosis (ORN) are not well studied regarding their correlations with nearby bone lesions. The aim of this study is to investigate the severity of radiation-induced STIs in advanced mandibular ORN and its relationship with hard-tissue damage and postoperative outcomes.
Methods: A retrospective study was performed in our institution from January 2017 to December 2019. Aside from demographic factors, the associations between the triad ORN variables (irradiation doses, ORN stages, ORN sizes) and radiation-related STI factors, vascular characteristics, and postoperative functional recovery were assessed. In addition, the severity of STI was also compared with treatment outcomes. Such correlations were established via both univariate and multivariable analyses.
Results: A total number of 47 patients were included. The median follow-up reached 27 months. Nasopharyngeal cancer was the histology type among most patients (n = 21, 44.7%). The median irradiation doses reached 62 Gy (range, 40-110 Gy). For STI, the symptom scoring equaled an average of 5.4 (range from 1 to 12), indicative of the severity of STI problems. During preoperative MRI examinations, signs of hypertrophy or edema (n = 41, 87.2%) were frequently discerned. Most patients (n = 23, 48.9%) also had extensive muscular fibrosis and infection, which required further debridement and scar release. Surprisingly, most STI factors, except cervical fibrosis (p = 0.02), were not in parallel with the ORN levels. Even the intraoperative soft-tissue defect changes could not be extrapolated by the extent of ORN damage (p = 0.096). Regarding the outcomes, a low recurrence rate (n = 3, 6.9%) was reported. In terms of soft tissue-related factors, we found a strong correlation (p = 0.004) between symptom scores and recurrence. In addition, when taking trismus into consideration, both improvements in mouth-opening distance (p < 0.001) and facial contour changes (p = 0.004) were adversely affected. Correlations were also observed between the intraoperative soft-tissue defect changes and complications (p = 0.024), indicative of the importance of STI evaluation and management.
Conclusions: The coexistence of hard- and soft-tissue damage in radiation-induced advanced mandibular ORN patients reminds surgeons of the significance in assessing both aspects. It is necessary to take the same active measures to evaluate and repair both severe STIs and ORN bone lesions.
Keywords: correlation; evaluation; fibrosis; management; osteoradionecrosis; risk; soft tissue injury; toxicity.
Copyright © 2021 Ma, Gao, Liu, Zhu, Zhu, Li and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- Sroussi HY, Epstein JB, Bensadoun RJ, Saunders DP, Lalla RV, Migliorati CA, et al. . Common oral complications of head and neck cancer radiation therapy: mucositis, infections, saliva change, fibrosis, sensory dysfunctions, dental caries, periodontal disease, and osteoradionecrosis. Cancer Med (2017) 6(12):2918–31. 10.1002/cam4.1221 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources