

Performance of PRISM III, PELOD-2, and P-MODS Scores in Two Pediatric Intensive Care Units in China
- PMID: 33996681
- PMCID: PMC8113391
- DOI: 10.3389/fped.2021.626165
Performance of PRISM III, PELOD-2, and P-MODS Scores in Two Pediatric Intensive Care Units in China
Abstract
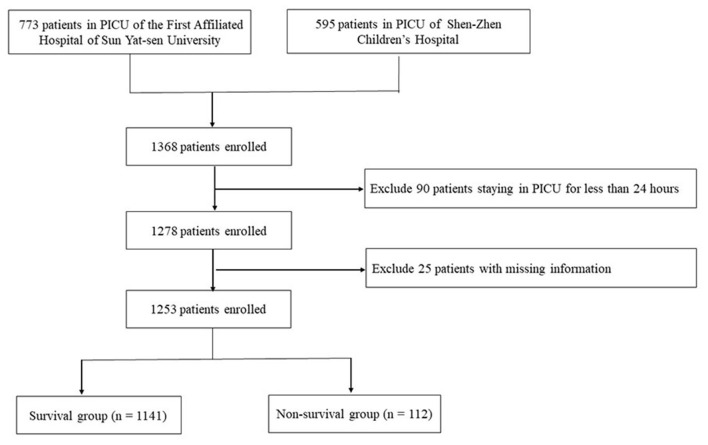
Objective: The performances of the pediatric risk of mortality score III (PRISM III), pediatric logistic organ dysfunction score-2 (PELOD-2), and pediatric multiple organ dysfunction score (P-MODS) in Chinese patients are unclear. This study aimed to assess the performances of these scores in predicting mortality in critically ill pediatric patients. Methods: This retrospective observational study was conducted at two tertiary-care PICUs of teaching hospitals in China. A total of 1,253 critically ill pediatric patients admitted to the two Pediatric Intensive Care Units (PICUs) of the First Affiliated Hospital, Sun Yat-Sen University from August 2014 to December 2019 and Shen-Zhen Children's Hospital from January 2019 to December 2019 were analyzed. The indexes of discrimination and calibration were applied to evaluate score performance for the three models (PRISM III, PELOD-2, and P-MODS scores). The receiver operating characteristic (ROC) curve was plotted, and the efficiency of PRISM III, PELOD-2, and P-MODS in predicting death were evaluated by the area under ROC curve (AUC). Hosmer-Lemeshow goodness-of-fit test was used to evaluate the degree of fitting between the mortality predictions of each scoring system and the actual mortality. Results: A total of 1,253 pediatric patients were eventually enrolled in this study (median age, 38 months; overall mortality rate, 8.9%; median length of PICU stay, 8 days). Compared to the survival group, the non-survival group showed significantly higher PRISM III, PELOD-2, and P-MODS scores [PRISM III: 18 (12, 23) vs. 11 (0, 16); PELOD-2, 8 (4, 10) vs. 4 (0, 6); and P-MODS: 5 (4, 9) vs. 3 (0, 4), all P < 0.001]. ROC curve analysis showed that the AUCs of PRISM III, PELOD-2, and P-MODS for predicting the death of critically ill children were 0.858, 0.721, and 0.596, respectively. Furthermore, in the Hosmer-Lemeshow goodness-of-fit test, PRISM III and PELOD-2 showed the better calibration between predicted mortality and observed mortality (PRISM III: χ2 = 5.667, P = 0.368; PELOD-2: χ2 = 9.582, P = 0.276; P-MODS: χ2 = 12.449, P = 0.015). Conclusions: PRISM III and PELOD-2 can discriminate well between survivors and non-survivors. PRISM III and PELOD-2 showed the better calibration between predicted and observed mortality, while P-MODS showed poor calibration.
Keywords: cohort study; mortality; pediatric intensive care unit; prediction; prognostic score.
Copyright © 2021 Zhang, Wu, Huang, Liu, Cheng, Xu, Tang and Luo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Predictive value of four pediatric scores of critical illness and mortality on evaluating mortality risk in pediatric critical patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018 Jan;30(1):51-56. doi: 10.3760/cma.j.issn.2095-4352.2018.01.010. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018. PMID: 29308758 Chinese.
-
Performance of PRISM III and PELOD-2 scores in a pediatric intensive care unit.Eur J Pediatr. 2015 Oct;174(10):1305-10. doi: 10.1007/s00431-015-2533-5. Epub 2015 Apr 15. Eur J Pediatr. 2015. PMID: 25875250
-
Performance of the PRISM I, PIM2, PELOD-2 and PRISM IV scoring systems in western China: a multicenter prospective study.World J Pediatr. 2022 Dec;18(12):818-824. doi: 10.1007/s12519-022-00603-8. Epub 2022 Sep 13. World J Pediatr. 2022. PMID: 36100796
-
Meta-Analysis for the Prediction of Mortality Rates in a Pediatric Intensive Care Unit Using Different Scores: PRISM-III/IV, PIM-3, and PELOD-2.Front Pediatr. 2021 Aug 24;9:712276. doi: 10.3389/fped.2021.712276. eCollection 2021. Front Pediatr. 2021. PMID: 34504815 Free PMC article.
-
Clinical prognostic models in children with sepsis in low- and middle-income countries: a systematic review and meta-analysis.Front Pediatr. 2024 Oct 17;12:1463986. doi: 10.3389/fped.2024.1463986. eCollection 2024. Front Pediatr. 2024. PMID: 39483529 Free PMC article.
Cited by
-
A nomogram to predict 28-day mortality in neonates with sepsis: a retrospective study based on the MIMIC-III database.Transl Pediatr. 2023 Sep 18;12(9):1690-1706. doi: 10.21037/tp-23-150. Epub 2023 Sep 5. Transl Pediatr. 2023. PMID: 37814720 Free PMC article.
-
[Clinical sub-phenotypes of acute kidney injury in children and their association with prognosis].Zhongguo Dang Dai Er Ke Za Zhi. 2025 Jan 15;27(1):47-54. doi: 10.7499/j.issn.1008-8830.2408060. Zhongguo Dang Dai Er Ke Za Zhi. 2025. PMID: 39825651 Free PMC article. Chinese.
-
Prediction of urinary dickkopf-3 for AKI, sepsis-associated AKI, and PICU mortality in children.Pediatr Res. 2023 May;93(6):1651-1658. doi: 10.1038/s41390-022-02269-4. Epub 2022 Aug 25. Pediatr Res. 2023. PMID: 36008594
-
Predicting functional and quality-of-life outcomes following pediatric sepsis: performance of PRISM-III and PELOD-2.Pediatr Res. 2023 Dec;94(6):1951-1957. doi: 10.1038/s41390-023-02619-w. Epub 2023 Apr 26. Pediatr Res. 2023. PMID: 37185949 Free PMC article.
-
The relationship between lactate/albumin ratio and prognosis in children with acute kidney injury.PLoS One. 2025 Aug 1;20(8):e0329453. doi: 10.1371/journal.pone.0329453. eCollection 2025. PLoS One. 2025. PMID: 40748973 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources