

Survival and Complication of Liver Transplantation in Infants: A Systematic Review and Meta-Analysis
- PMID: 33996682
- PMCID: PMC8116516
- DOI: 10.3389/fped.2021.628771
Survival and Complication of Liver Transplantation in Infants: A Systematic Review and Meta-Analysis
Abstract
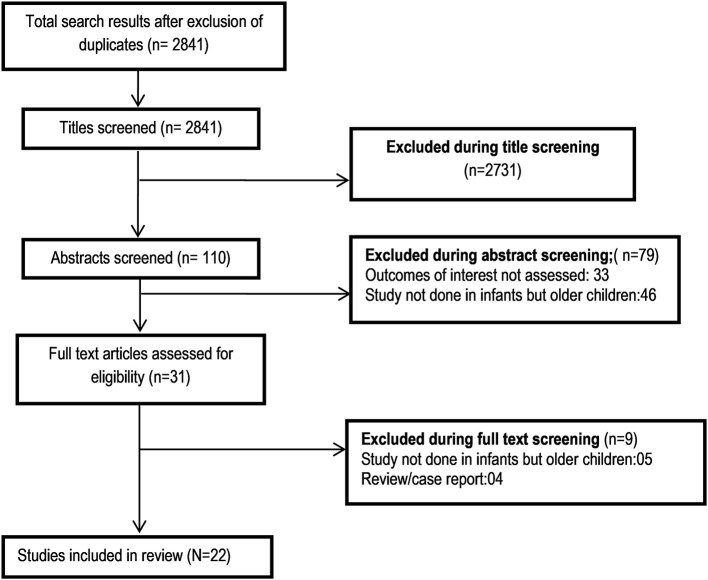
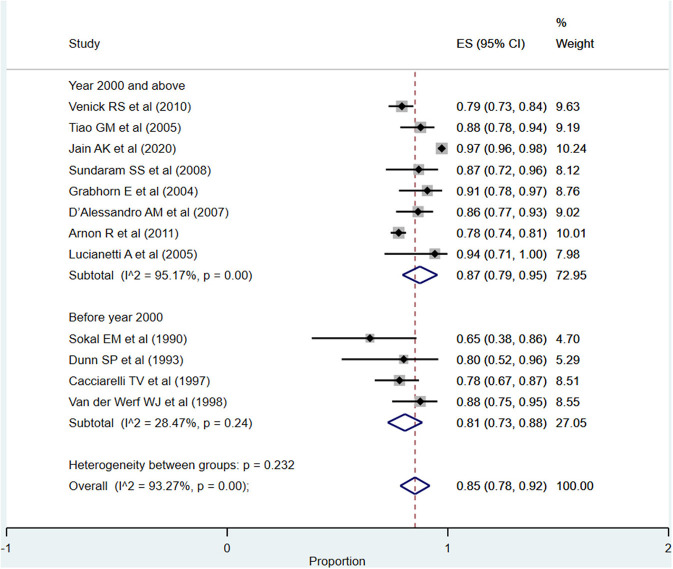
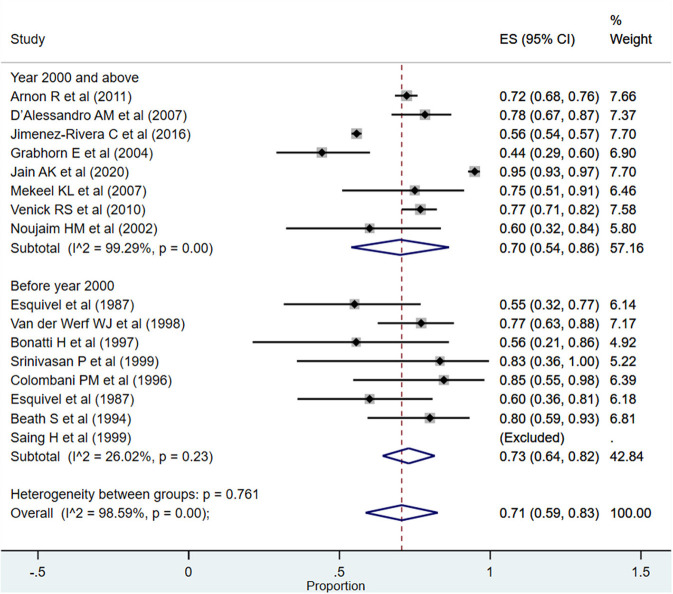
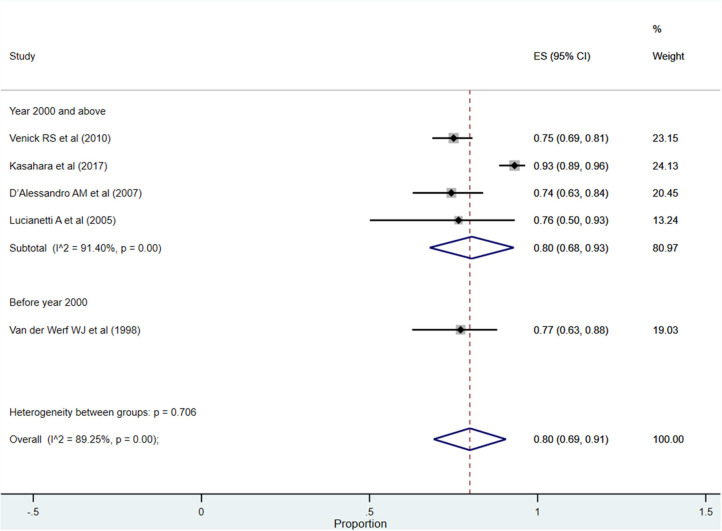
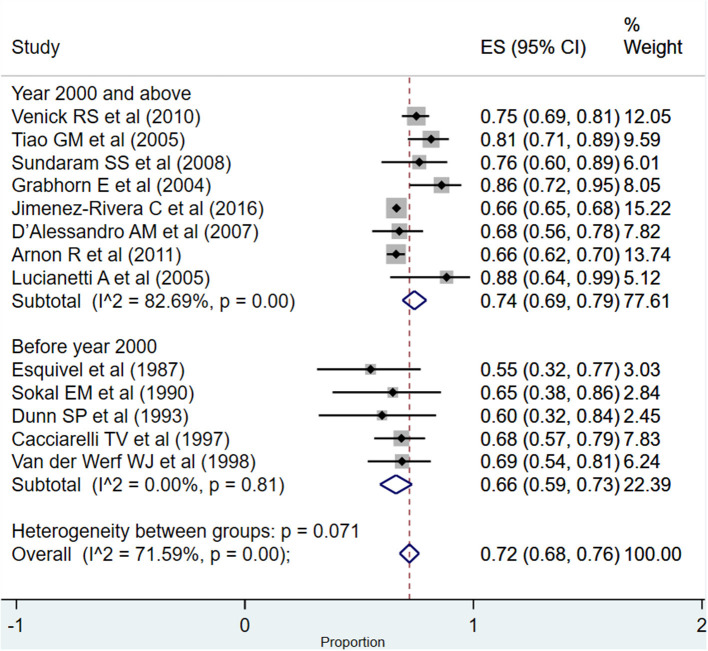
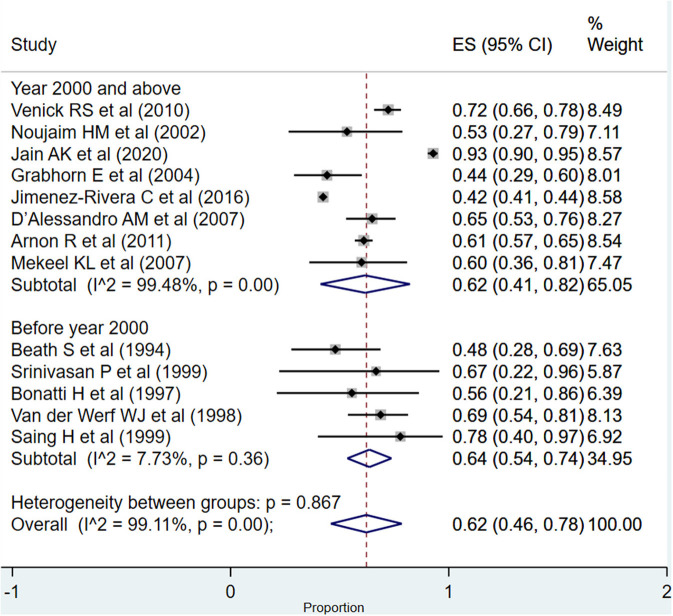
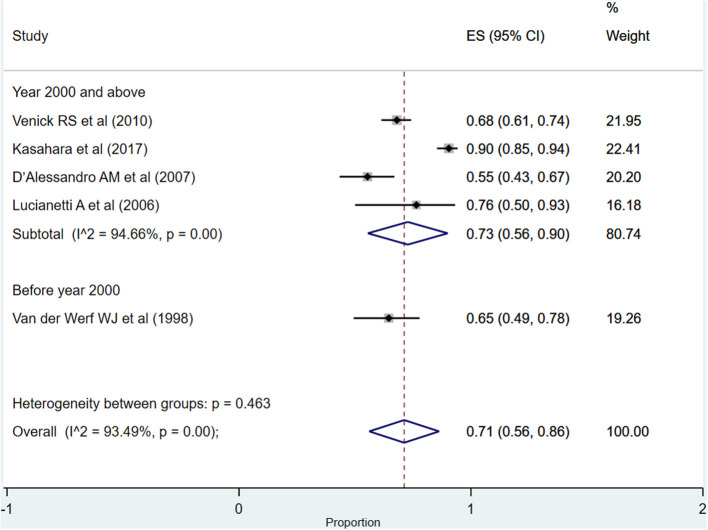
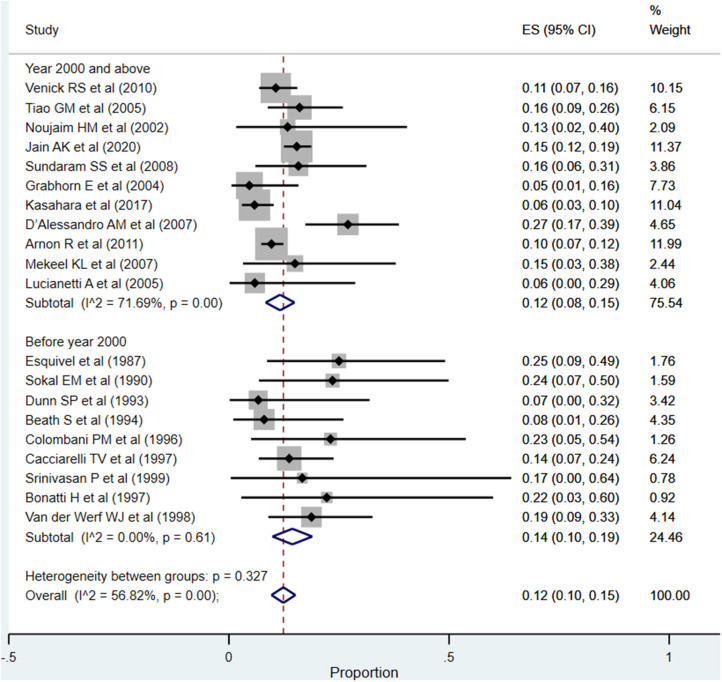
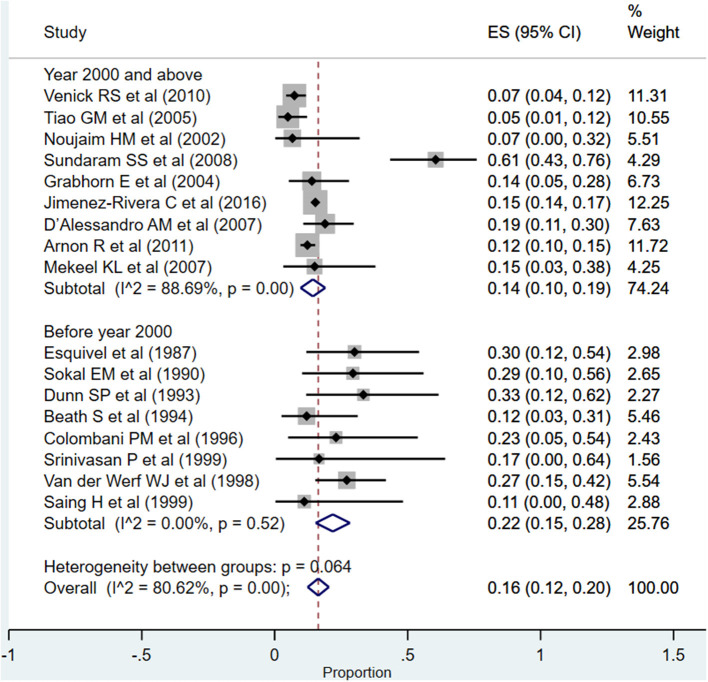
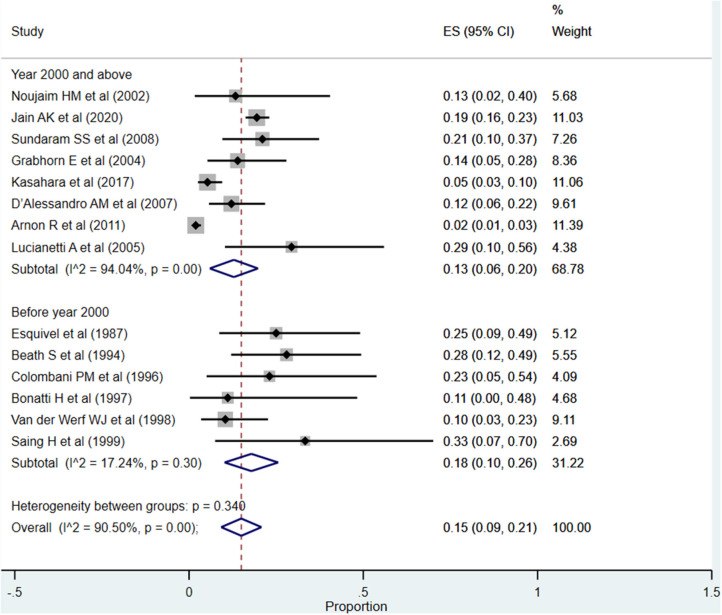
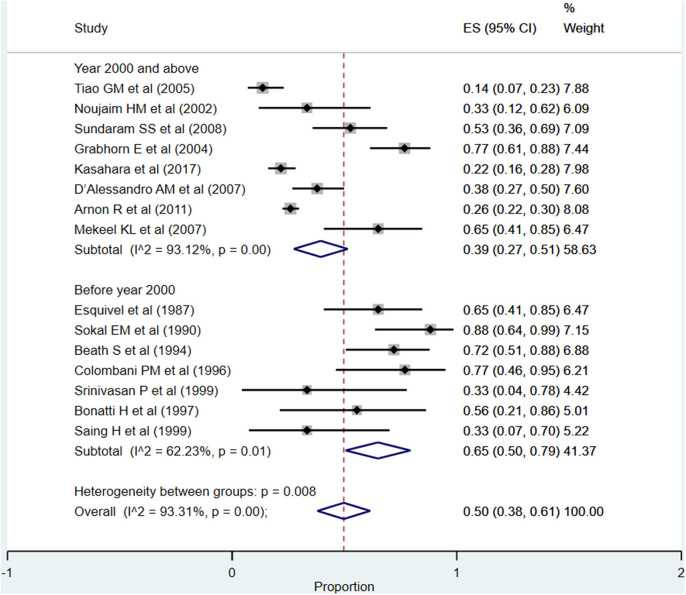
Background: Modern surgical techniques and scientific advancements have made liver transplant (LT) in infants feasible. However, there are only a small number of studies examining the short- as well as long-term outcomes of LT in this vulnerable subset of children. Methods: Comprehensive searches were done systematically through the PubMed, Scopus, and Google scholar databases. Studies that were retrospective record based or adopted a cohort approach and reported either patient survival rates or graft survival rates or complications of LT in infants were included in the meta-analysis. Statistical analysis was done using STATA version 13.0. Results: A total of 22 studies were included in the meta-analysis. The overall pooled patient survival rate at 1 year, >1-5 years, and >5 years post-transplantation was 85% (95% CI: 78--92%), 71% (95% CI: 59-83%), and 80% (95% CI: 69-91%), respectively. The overall pooled graft survival rate at 1 year, >1-5 years, and >5 years post-transplantation was 72% (95% CI: 68-76%), 62% (95% CI: 46-78%), and 71% (95% CI: 56-86%), respectively. The overall pooled rate for vascular complications, need for re-transplantation, biliary complications, and infection/sepsis was 12% (95% CI: 10-15%), 16% (95% CI: 12-20%), 15% (95% CI: 9-21%), and 50% (95% CI: 38-61%), respectively. Conclusion: The current meta-analysis showed modest patient and graft survival rates for infant liver transplantation. However, the complication rates related to infection/sepsis were high. More comprehensive evidence is required from studies with larger sample sizes and a longer duration of follow-up.
Keywords: complication; infants; liver transplant; meta-analysis; survival.
Copyright © 2021 Hou, Wang, Yang and Zhong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Comparison of clinical outcomes between ABO-incompatible and ABO-compatible pediatric liver transplantation: a systematic literature review and meta-analysis.Pediatr Surg Int. 2020 Nov;36(11):1353-1362. doi: 10.1007/s00383-020-04746-5. Epub 2020 Oct 1. Pediatr Surg Int. 2020. PMID: 33001256
-
Outcomes after liver transplantation in young infants.J Pediatr Gastroenterol Nutr. 2008 Oct;47(4):486-92. doi: 10.1097/MPG.0b013e318175d7d2. J Pediatr Gastroenterol Nutr. 2008. PMID: 18852642
-
The Association of obesity with vascular complications after liver transplantation.BMC Gastroenterol. 2019 Mar 7;19(1):39. doi: 10.1186/s12876-019-0954-8. BMC Gastroenterol. 2019. PMID: 30845923 Free PMC article.
-
Liver transplantation in very small infants.Pediatr Transplant. 2007 Feb;11(1):66-72. doi: 10.1111/j.1399-3046.2006.00610.x. Pediatr Transplant. 2007. PMID: 17239125
-
Atrial fibrillation in renal or liver transplant recipients: A systematic review and meta-analysis.Transplant Rev (Orlando). 2019 Jan;33(1):29-38. doi: 10.1016/j.trre.2018.07.003. Epub 2018 Aug 9. Transplant Rev (Orlando). 2019. PMID: 30139706
Cited by
-
CREB1 and PPAR-α/γ Pathways in Hepatic Ischemia/Reperfusion: Route for Curcumin to Hepatoprotection.Iran J Pharm Res. 2023 Feb 1;21(1):e133779. doi: 10.5812/ijpr-133779. eCollection 2022 Dec. Iran J Pharm Res. 2023. PMID: 36942070 Free PMC article.
-
Differences in Physical Activity Levels between Healthy and Transplanted Children: Who Needs More Tips?Healthcare (Basel). 2023 May 31;11(11):1610. doi: 10.3390/healthcare11111610. Healthcare (Basel). 2023. PMID: 37297751 Free PMC article.
-
Preliminary Evaluation of Sedentary Lifestyle in Italian Children after Solid Transplant: What Role Could Physical Activity Play in Health? It Is Time to Move.Int J Environ Res Public Health. 2023 Jan 5;20(2):990. doi: 10.3390/ijerph20020990. Int J Environ Res Public Health. 2023. PMID: 36673745 Free PMC article.
-
The global survival rate of graft and patient in kidney transplantation of children: a systematic review and meta-analysis.BMC Pediatr. 2022 Aug 24;22(1):503. doi: 10.1186/s12887-022-03545-2. BMC Pediatr. 2022. PMID: 36002803 Free PMC article.
-
Recipient-associated risk factors for post-liver transplantation biliary complications: A cohort study.Indian J Gastroenterol. 2024 Aug;43(4):791-798. doi: 10.1007/s12664-023-01479-w. Epub 2024 Jan 3. Indian J Gastroenterol. 2024. PMID: 38172464
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources