

Clinical Outcomes of Arthroscopic Tenodesis Versus Tenotomy for Long Head of the Biceps Tendon Lesions: A Systematic Review and Meta-analysis of Randomized Clinical Trials and Cohort Studies
- PMID: 33997057
- PMCID: PMC8071980
- DOI: 10.1177/2325967121993805
Clinical Outcomes of Arthroscopic Tenodesis Versus Tenotomy for Long Head of the Biceps Tendon Lesions: A Systematic Review and Meta-analysis of Randomized Clinical Trials and Cohort Studies
Abstract
Background: Controversy exists concerning whether tenotomy or tenodesis is the optimal surgical treatment option for proximal biceps tendon lesions.
Purpose: To evaluate the clinical outcomes after arthroscopic tenodesis and tenotomy in the treatment of long head of the biceps tendon (LHBT) lesions.
Study design: Systematic review; Level of evidence, 4.
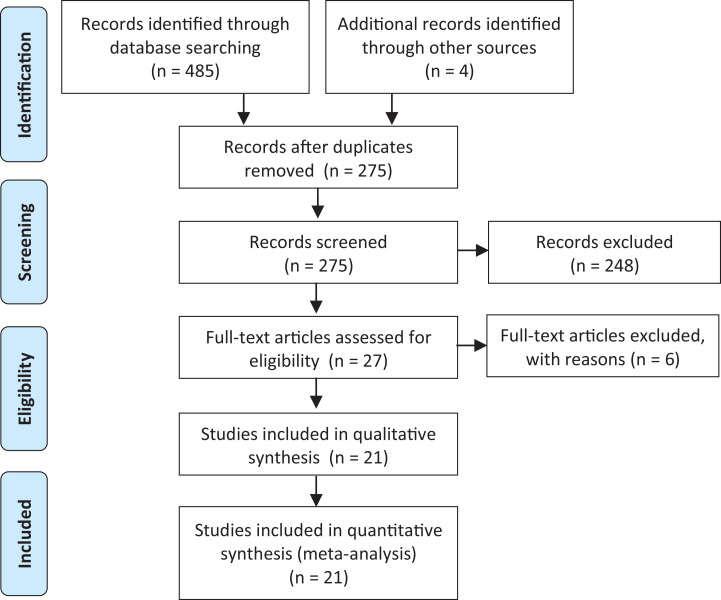
Methods: A systematic review was performed by searching PubMed, the Cochrane Library, Web of Science, and Embase to identify randomized controlled trials (RCTs) and cohort studies that compared the clinical efficacy of tenotomy with that of tenodesis for LHBT lesions. A standardized data extraction form was predesigned to obtain bibliographic information of the study as well as patient, intervention, comparison, and outcome data. A random-effects model was used to pool quantitative data from the primary outcomes.
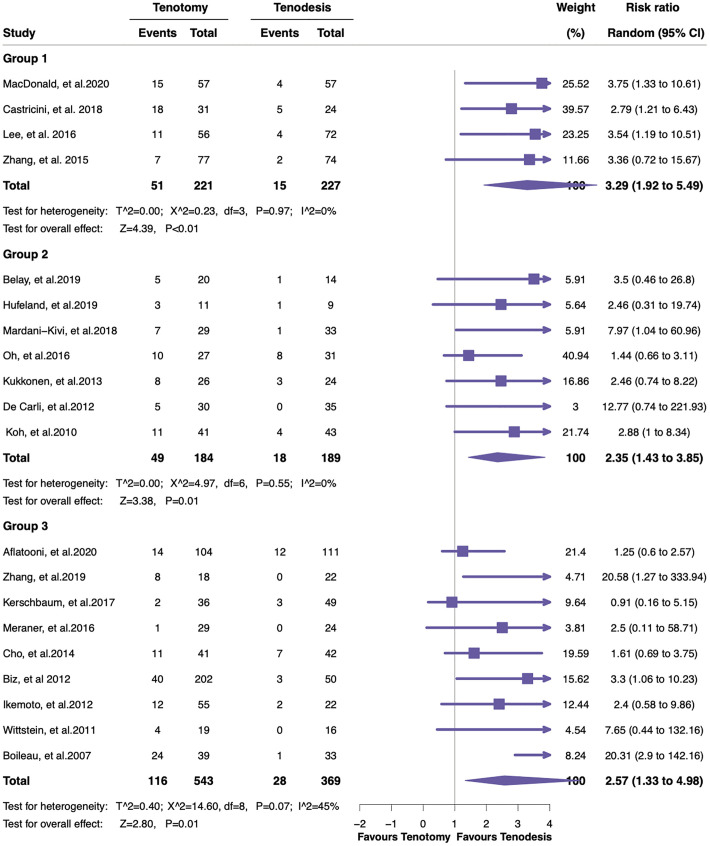
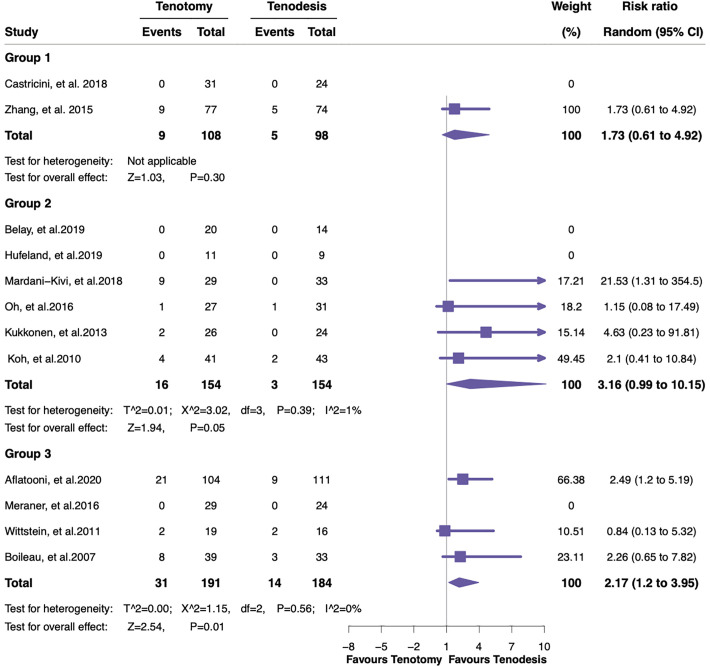
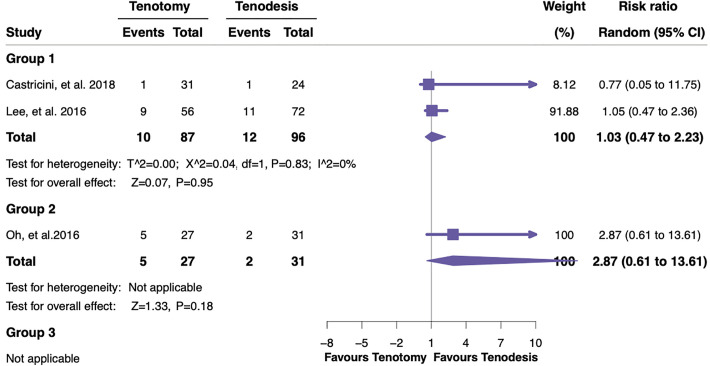
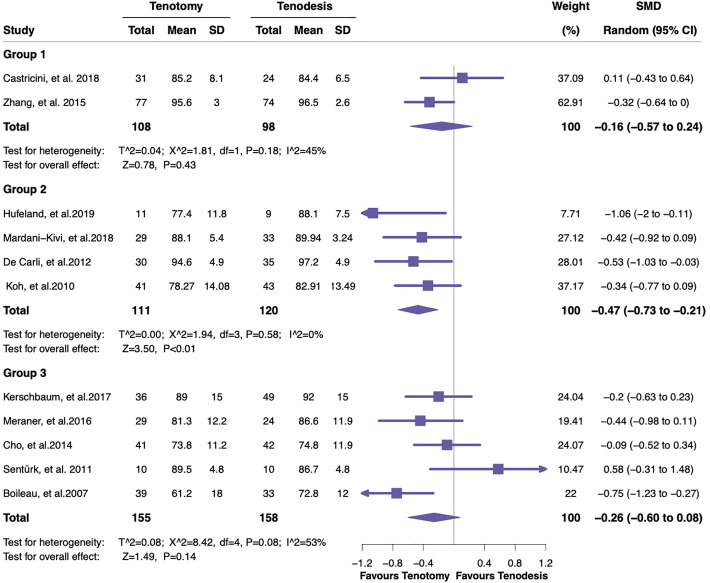
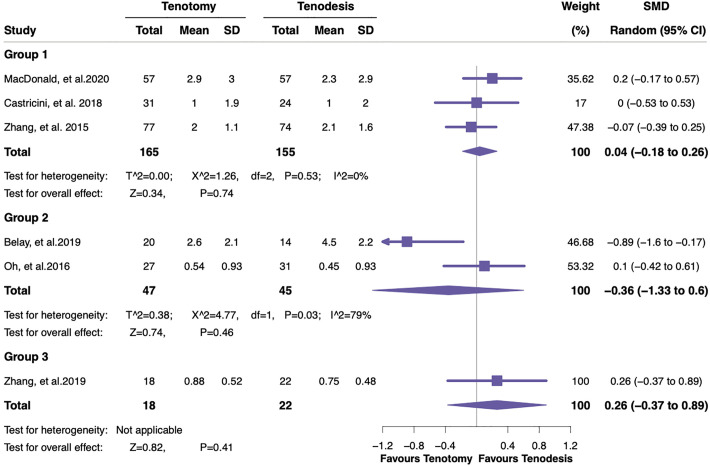
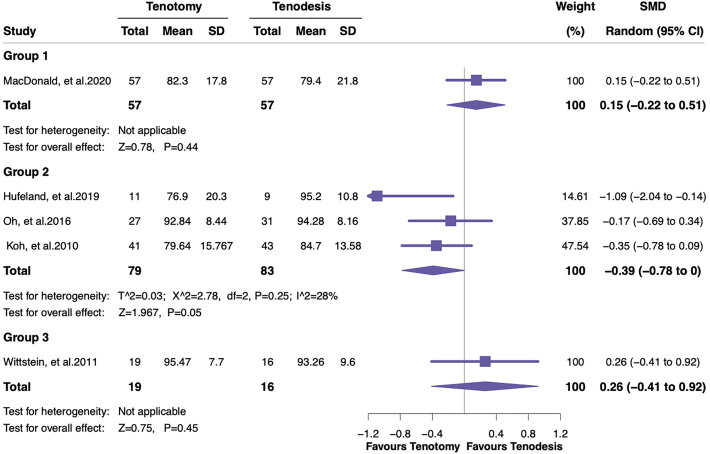
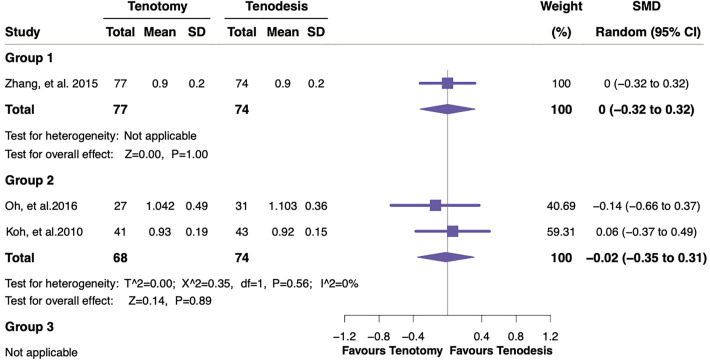
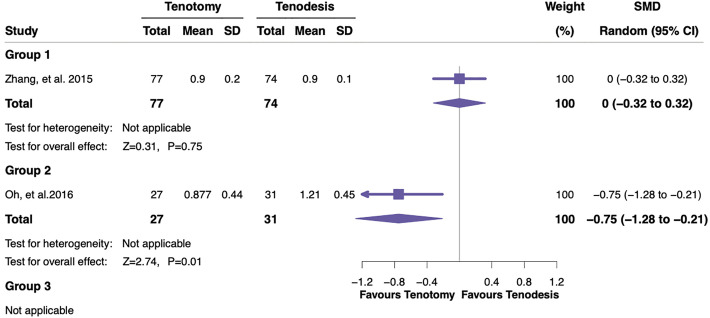
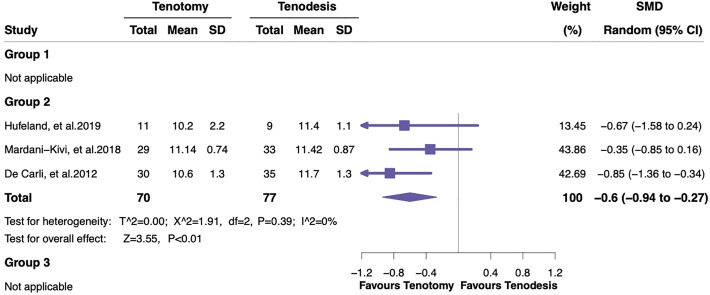
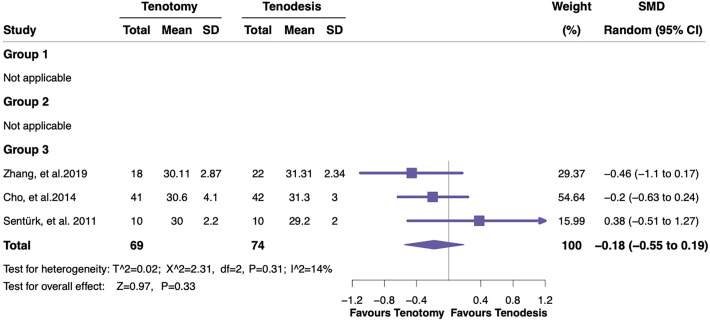
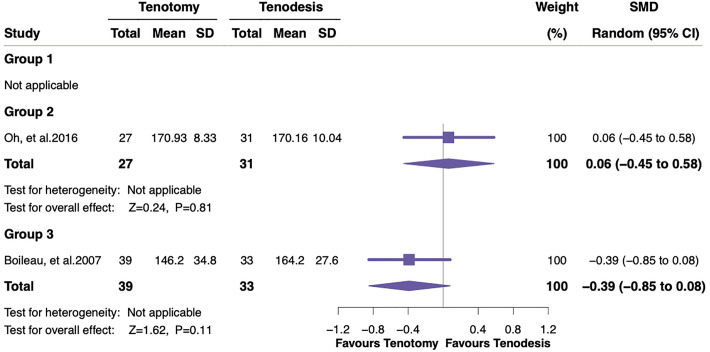
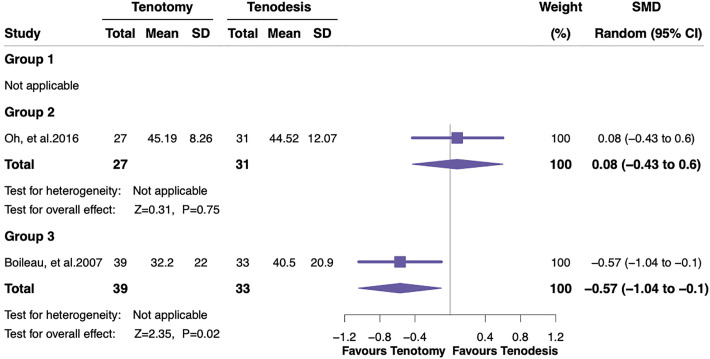
Results: A total of 21 eligible studies were separated into 3 methodological groups: (1) 4 RCTs with level 1 evidence, (2) 3 RCTs and 4 prospective cohort studies with level 2 evidence, and (3) 10 retrospective cohort studies with level 3 to 4 evidence. Analysis of the 3 groups demonstrated a significantly higher risk of the Popeye sign after tenotomy versus tenodesis (group 1: risk ratio [RR], 3.29 [95% CI, 1.92-5.49]; group 2: RR, 2.35 [95% CI, 1.43-3.85]; and group 3: RR, 2.57 [95% CI, 1.33-4.98]). Arm cramping pain remained significantly higher after tenotomy only in the retrospective cohort group (RR, 2.17 [95% CI, 1.20-3.95]). The Constant score for tenotomy was significantly worse than that for tenodesis in the prospective cohort group (standardized mean difference [SMD], -0.47 [95% CI, -0.73 to -0.21]), as were the forearm supination strength index (SMD, -0.75 [95% CI, -1.28 to -0.21]) and the Simple Shoulder Test (SST) score (SMD, -0.60 [95% CI, -0.94 to -0.27]).
Conclusion: The results demonstrated that compared with tenodesis, tenotomy had a higher risk of a Popeye deformity in all 3 study groups; worse functional outcomes in terms of the Constant score, forearm supination strength index, and SST score according to prospective cohort studies; and a higher incidence of arm cramping pain according to retrospective cohort studies.
Keywords: Biceps; arthroscopic; meta-analysis; tenodesis; tenotomy.
© The Author(s) 2021.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Beijing Municipal Science and Technology Commission (grant Z171100001017209), National Natural Science Foundation of China (grants 81972130, 81703896, 81972107, 81902203, and 82072494), National Key Research and Development Program of China (grant 2017YFC0108102), and Capital Health Research and Development of Special Fund (grant 2020-2-4067). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Ahmad CS, ElAttrache NS. Arthroscopic biceps tenodesis. Orthop Clin North Am. 2003;34(4):499–506. - PubMed
-
- Belay ES, Wittstein JR, Garrigues GE, et al. Biceps tenotomy has earlier pain relief compared to biceps tenodesis: a randomized prospective study. Knee Surg Sports Traumatol Arthrosc. 2019;27(12):4032–4037. - PubMed
-
- Boileau P, Baque F, Valerio L, Ahrens P, Chuinard C, Trojani C. Isolated arthroscopic biceps tenotomy or tenodesis improves symptoms in patients with massive irreparable rotator cuff tears. J Bone Joint Surg Am. 2007;89:747–757. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
