

Do Narcotic Use, Physical Therapy Location, or Payer Type Predict Patient-Reported Outcomes After Anterior Cruciate Ligament Reconstruction?
- PMID: 33997058
- PMCID: PMC8085373
- DOI: 10.1177/2325967121994833
Do Narcotic Use, Physical Therapy Location, or Payer Type Predict Patient-Reported Outcomes After Anterior Cruciate Ligament Reconstruction?
Abstract
Background: Opioid use and public insurance have been correlated with worse outcomes in a number of orthopaedic surgeries. These factors have not been investigated with anterior cruciate ligament reconstruction (ACLR).
Purpose/hypothesis: To evaluate if narcotic use, physical therapy location, and insurance type are predictors of patient-reported outcomes after ACLR. It was hypothesized that at 1 year postsurgically, increased postoperative narcotic use would be associated with worse outcomes, physical therapy obtained within the authors' integrated health care system would lead to better outcomes, and public insurance would lead to worse outcomes and athletic activity.
Study design: Cohort study; Level of evidence, 2.
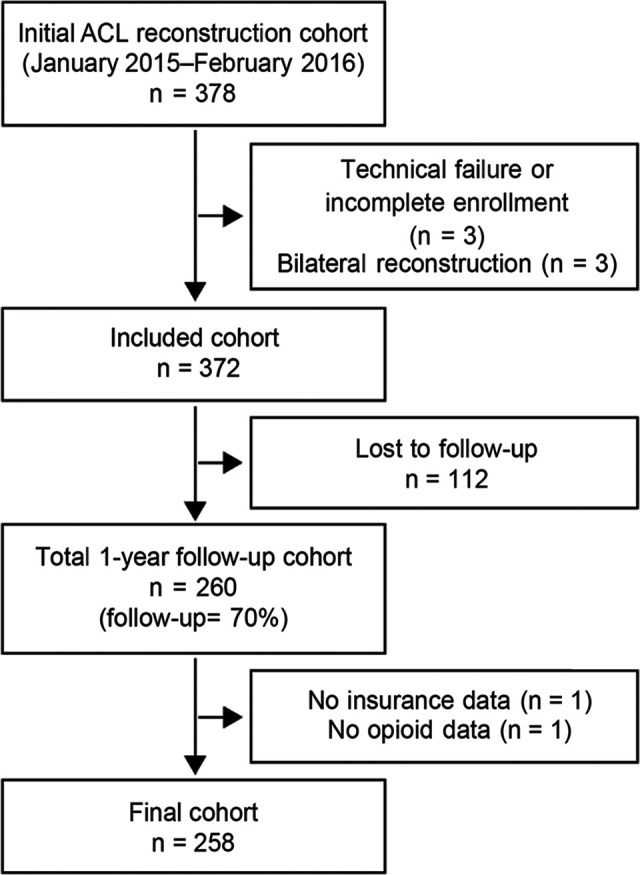
Methods: All patients undergoing unilateral, primary ACLR between January 2015 and February 2016 at a large health system were enrolled in a standard-of-care prospective cohort. Knee injury and Osteoarthritis Score (KOOS) and the Hospital for Special Surgery Pediatric-Functional Activity Brief Scale (HSS Pedi-FABS) were collected before surgery and at 1 year postoperatively. Concomitant knee pathology was assessed arthroscopically and electronically captured. Patient records were analyzed to determine physical therapy location, insurance status, and narcotic use. Multivariable regression analyses were used to identify significant predictors of the KOOS and HSS Pedi-FABS score.
Results: A total of 258 patients were included in the analysis (mean age, 25.8; 51.2% women). In multivariable regression analysis, narcotic use, physical therapy location, and insurance type were not independent predictors of any KOOS subscales. Public insurance was associated with a lower HSS Pedi-FABS score (-4.551, P = .047) in multivariable analysis. Narcotic use or physical therapy location was not associated with the HSS Pedi-FABS score.
Conclusion: Increased narcotic use surrounding surgery, physical therapy location within the authors' health care system, and public versus private insurance were not associated with disease-specific KOOS subscale scores. Patients with public insurance had worse HSS Pedi-FABS activity scores compared with patients with private insurance, but neither narcotic use nor physical therapy location was associated with activity scores. Physical therapy location did not influence outcomes, suggesting that patients be given a choice in the location they received physical therapy (as long as a standardized protocol is followed) to maximize compliance.
Keywords: HSS Pedi-FABS; KOOS; anterior cruciate ligament reconstruction; opioid use; payer status.
© The Author(s) 2021.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: Research reported in this publication was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health (award K23AR066133), which supported a portion of M.H.J.’s professional effort. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. L.D.F. has received consulting fees from Zimmer Biomet and hospitality payments from Musculoskeletal Transplant Foundation. M.H.J. is on the scientific advisory board for Samumed. A.A.M. has received educational support from Rock Medical; consulting fees from Arthrosurface, Amniox Medical, Linvatec, Stryker, and Trice; speaking fees from Trice; royalties from Arthrosurface, Zimmer Biomet, and Wolters Kluwer; and hospitality payments from Arthrex, DJO, and Smith & Nephew; and has stock/stock options in Arthrosurface and Trice. R.D.P. has received royalties from Zimmer Biomet and hospitality payments from Smith & Nephew and Musculoskeletal Transplant Foundation. J.T.R. has received consulting fees from Smith & Nephew. P.S. has received educational support from Rock Medical; consulting fees from Arthrex, DJO, and DePuy; speaking fees from Arthrex; and hospitality payments from Musculoskeletal Transplant Foundation. G.S. has received royalties from Oberd. K.P.S. has received research support from Smith & Nephew and DJO; consulting fees from NFL, Cytori, Mitek, Samumed, and Flexion Therapeutics; hospitality payments from DePuy and Biosense Webster; and royalties from Oberd. J.S.W. has received educational support from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
Association of Grit With Postoperative Knee Outcomes and Physical Function After ACL Reconstruction in Adolescent Athletes.Am J Sports Med. 2023 Sep;51(11):2900-2907. doi: 10.1177/03635465231187040. Epub 2023 Jul 31. Am J Sports Med. 2023. PMID: 37525482
-
Time interval affects physical activity scores: a comparison of the Marx Activity Rating Scale and the Hospital for Special Surgery Pediatric Functional Activity Brief Scale.Knee Surg Sports Traumatol Arthrosc. 2020 Aug;28(8):2619-2625. doi: 10.1007/s00167-020-05895-9. Epub 2020 Feb 19. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 32076731
-
An Activity Scale for All Youth Athletes? Clinical Considerations for the HSS Pedi-FABS.Orthop J Sports Med. 2022 Dec 22;10(12):23259671221143534. doi: 10.1177/23259671221143534. eCollection 2022 Dec. Orthop J Sports Med. 2022. PMID: 36582933 Free PMC article.
-
A Modified Lemaire Lateral Extra-articular Tenodesis in High-Risk Adolescents Undergoing Anterior Cruciate Ligament Reconstruction With Quadriceps Tendon Autograft: 2-Year Clinical Outcomes.Am J Sports Med. 2023 May;51(6):1441-1446. doi: 10.1177/03635465231160681. Epub 2023 Mar 14. Am J Sports Med. 2023. PMID: 36917840
-
Are articular cartilage lesions and meniscus tears predictive of IKDC, KOOS, and Marx activity level outcomes after anterior cruciate ligament reconstruction? A 6-year multicenter cohort study.Am J Sports Med. 2014 May;42(5):1058-67. doi: 10.1177/0363546514525910. Epub 2014 Mar 19. Am J Sports Med. 2014. PMID: 24647881 Free PMC article.
Cited by
-
The posterior cruciate ligament index as a reliable indirect sign of anterior cruciate ligament rupture is associated with the course of knee joint injury.Knee Surg Sports Traumatol Arthrosc. 2023 Aug;31(8):3277-3283. doi: 10.1007/s00167-023-07357-4. Epub 2023 Mar 11. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 36899193
References
-
- Anthony C, Westermann RW, Bedard N, et al. Opioid demand after anterior cruciate ligament reconstruction. Orthop J Sports Med. 2017;5(7)(suppl 6):2325967117S00278. - PubMed
-
- Anthony CA, Westermann RW, Bedard N, et al. Opioid demand before and after anterior cruciate ligament reconstruction. Am J Sports Med. 2017;45(13):3098–3103. - PubMed
-
- Ardern CL, Sonesson S, Forssblad M, Kvist J. Comparison of patient-reported outcomes among those who chose ACL reconstruction or non-surgical treatment. Scand J Med Sci Sports. 2017;27(5):535–544. - PubMed
-
- Armaghani SJ, Lee DS, Bible JE, et al. Preoperative opioid use and its association with perioperative opioid demand and postoperative opioid independence in patients undergoing spine surgery. Spine. 2014;39(25):e1524. - PubMed
-
- Barenius B, Ponzer S, Shalabi A, Bujak R, Norlén L, Eriksson K. Increased risk of osteoarthritis after anterior cruciate ligament reconstruction: a 14-year follow-up study of a randomized controlled trial. Am J Sports Med. 2014;42(5):1049–1057. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
