

Arthroscopic Management of Scapulothoracic Bursitis: Clinical Outcomes and Assessment of Novel Bony Parameters on Magnetic Resonance Imaging
- PMID: 33997061
- PMCID: PMC8085374
- DOI: 10.1177/2325967121998273
Arthroscopic Management of Scapulothoracic Bursitis: Clinical Outcomes and Assessment of Novel Bony Parameters on Magnetic Resonance Imaging
Abstract
Background: Scapulothoracic bursitis is a significant clinical condition that limits day-to-day function. Arthroscopic scapular debridement and resection have provided satisfactory outcomes; however, techniques, approaches, and recommendations remain varied. Novel bony parameters have also gained increasing interest owing to their value in preoperative planning.
Purpose: To assess midterm clinical outcomes after the arthroscopic management of scapulothoracic bursitis and to identify and measure novel bony parameters on preoperative magnetic resonance imaging.
Study design: Case series; Level of evidence, 4.
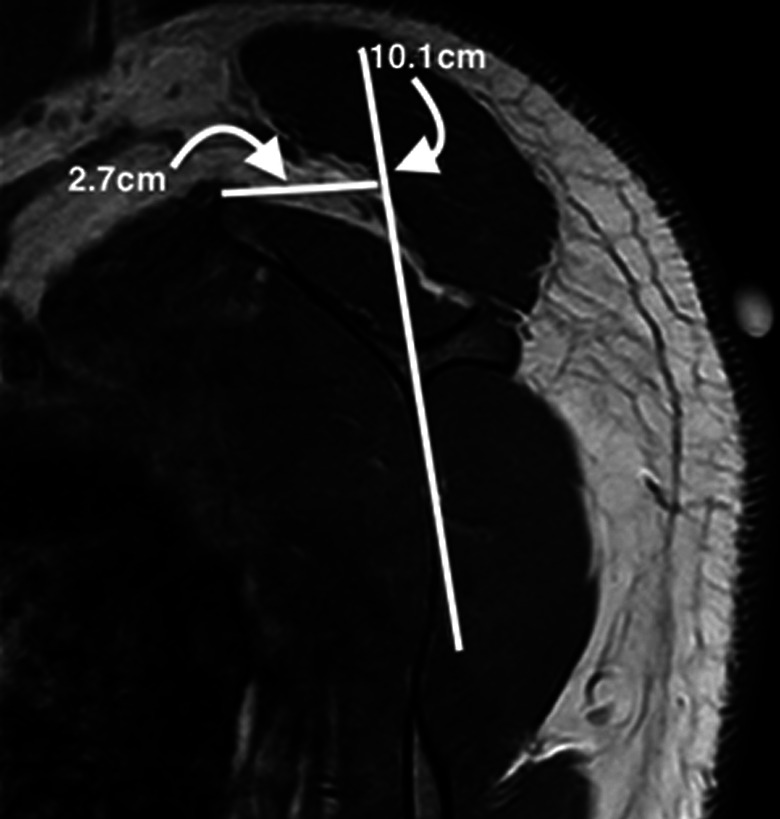
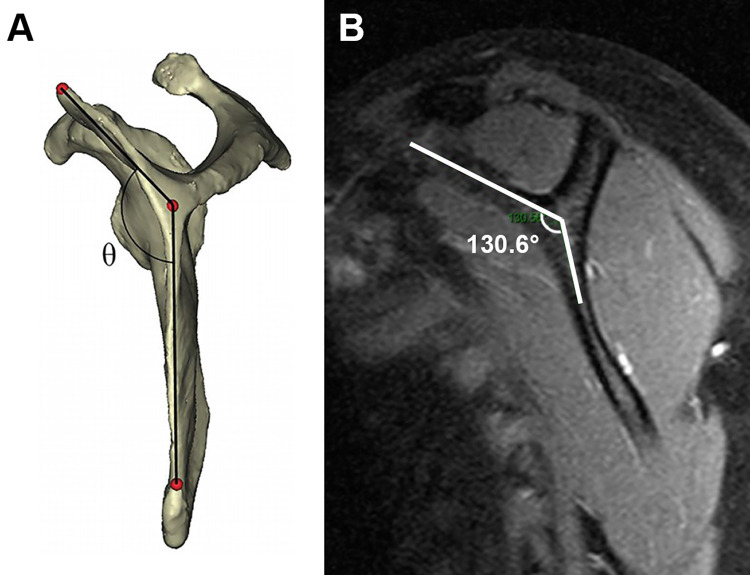
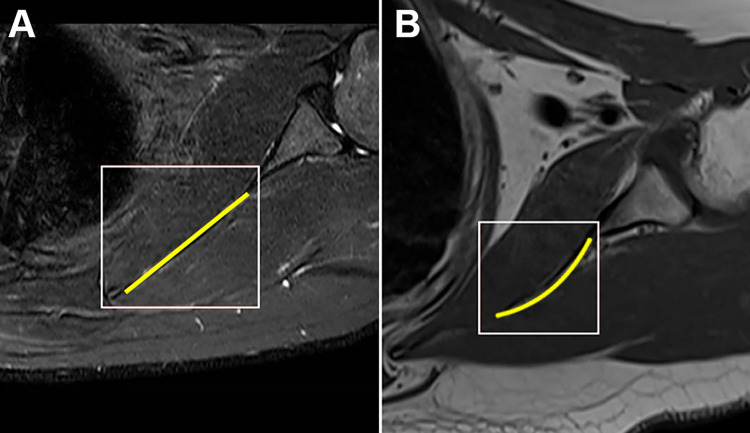
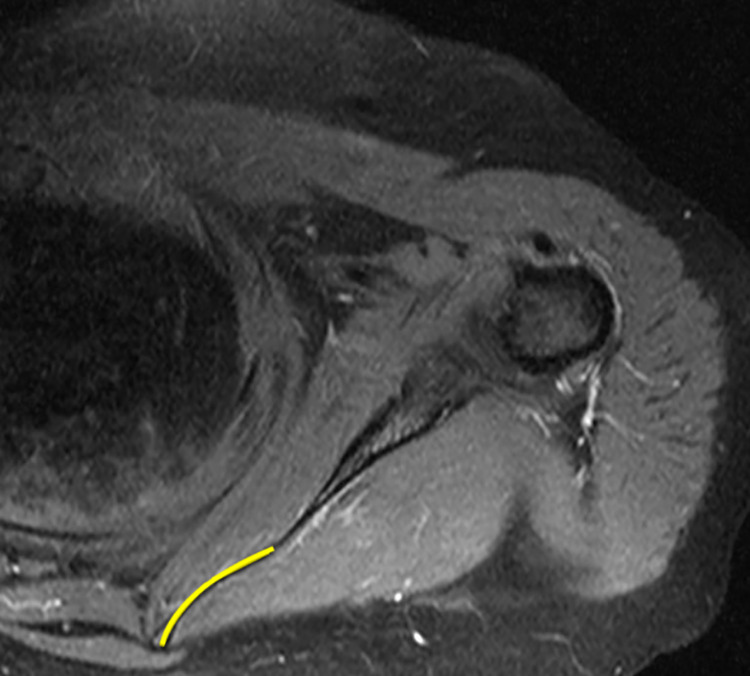
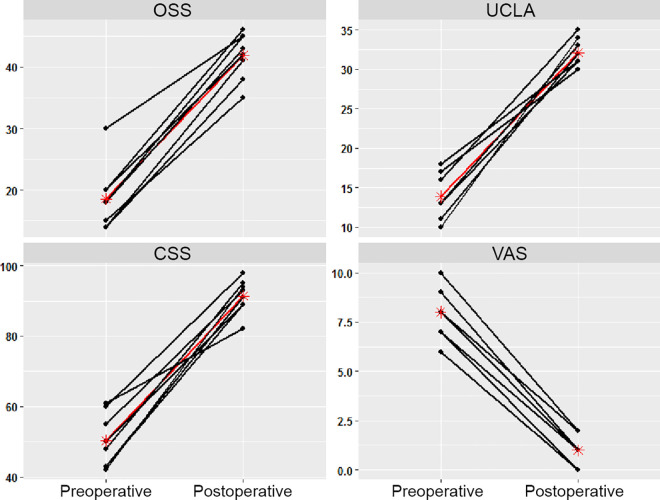
Methods: A total of 8 patients underwent arthroscopic scapular debridement and bursectomy; 5 of the 8 patients underwent additional medial scapulectomy. There were 5 male (62.5%) and 3 female (37.5%) patients with a mean age of 30.1 ± 12.3 years (range, 19-58 years). Inclusion criteria for surgery were patients with symptomatic scapulothoracic bursitis for whom extensive nonoperative modalities had been utilized for at least 6 months but failed. Outcome measures included the Oxford Shoulder Score (OSS), University of California Los Angeles (UCLA) shoulder rating scale, Constant Shoulder Score (CSS), and visual analog scale (VAS) for pain. The bony parameters included scapular shape, anterior offset, costomedial angle, and medial scapular corpus angle (MSCA).
Results: The follow-up duration was at least 2 years for all patients (mean follow-up, 25.0 ± 4.1 months [range, 24-35 months]). The majority of patients had a concave-shaped scapula (62.5%). The mean anterior offset was 24.3 ± 3.4 mm, and the mean costomedial angle was 132.3° ± 9.6°. Half the patients had a positive MSCA, while the other half had a negative MSCA. A statistically significant improvement was observed in the OSS, UCLA, CSS, and VAS scores from preoperatively to 2-year follow-up (P < .001 for all). No complications were observed.
Conclusion: Arthroscopic scapular debridement and resection provided satisfactory midterm clinical outcomes for the treatment of scapulothoracic bursitis.
Keywords: anterior offset; costomedial angle; scapulectomy; scapulothoracic bursitis; superomedial angle resection.
© The Author(s) 2021.
Conflict of interest statement
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Bell SN, Troupis JM, Miller D, Alta TD, Coghlan JA, Wijeratna MD. Four-dimensional computed tomography scans facilitate preoperative planning in snapping scapula syndrome. J Shoulder Elbow Surg. 2015;24(4):e83–e90. - PubMed
-
- Blønd L, Rechter S. Arthroscopic treatment for snapping scapula: a prospective case series. Eur J Orthop Surg Traumatol. 2014;24(2):159–164. - PubMed
-
- Chang WH, Kim YW, Choi S, Lee SC. Comparison of the therapeutic effects of intramuscular subscapularis and scapulothoracic bursa injections in patients with scapular pain: a randomized controlled trial. Rheumatol Int. 2014;34(9):1203–1209. - PubMed
-
- Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 1987;214:160–164. - PubMed
LinkOut - more resources
Full Text Sources
