

Incidence and Risk Factors for Residual High-Grade Pivot Shift After ACL Reconstruction With or Without a Lateral Extra-articular Tenodesis
- PMID: 33997078
- PMCID: PMC8113945
- DOI: 10.1177/23259671211003590
Incidence and Risk Factors for Residual High-Grade Pivot Shift After ACL Reconstruction With or Without a Lateral Extra-articular Tenodesis
Abstract
Background: Residual rotatory knee laxity at midterm follow-up after isolated anterior cruciate ligament reconstruction (ACLR) versus ACLR with lateral extra-articular tenodesis (LET) remains an issue.
Purpose/hypothesis: To evaluate the outcomes of ACLR with or without additional LET at a minimum 2-year follow-up in patients with preoperative high-grade pivot shift (PS). Our hypothesis was that the addition of LET would decrease the risk of secondary meniscal injury and the presence of residual high-grade PS at follow-up.
Study design: Cohort study; Level of evidence, 3.
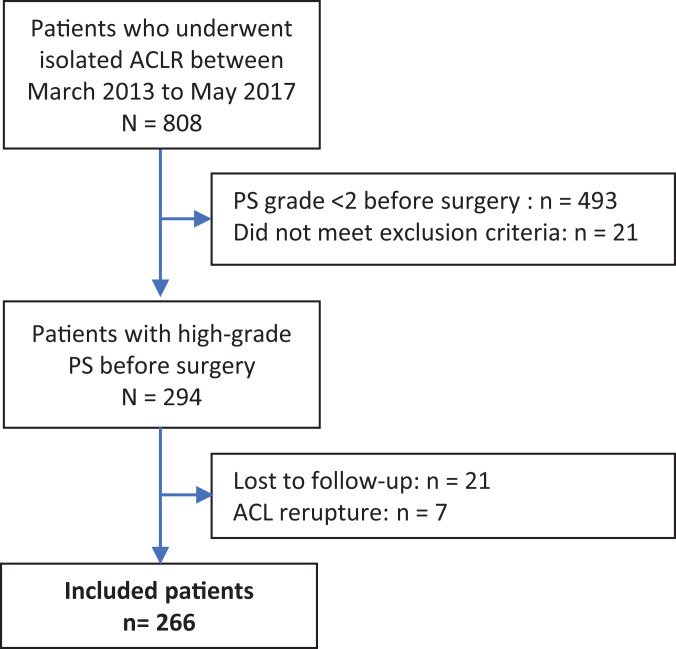
Methods: A retrospective analysis performed at 3 sports medicine centers identified 266 study patients; all had a high-grade PS (grade 2 or 3) preoperatively and underwent isolated ACLR with or without LET. Four different ACLR techniques were used: single-strand quadrupled semitendinosus (ST4) ACLR without LET (ST4 group; n = 55), ST4 with anatomic LET (ST4+LET group; n = 77), bone-patellar tendon and modified Lemaire LET (BTB+LET group; n = 43), and quadriceps tendon and modified Lemaire LET (QT+LET group; n = 91). At follow-up, we evaluated for the presence of high-grade (grade ≥2) PS. Preoperative meniscal tears and their treatment were recorded.
Results: Overall, 185 (69.5%) patients had at least 1 meniscal tear at index surgery. The mean follow-up period was 44.3 months; 47 (17.7%) patients had a new meniscal tear and 64 (24%) patients had a high-grade PS at follow-up. Compared with meniscal repair, significant predictors for high-grade PS at follow-up were meniscectomy (odds ratio [OR] = 2.65 [95% CI, 1.19-5.63]; P = .02) and nonrepair of preoperative meniscal tear (OR = 3.26 [95% CI, 1.27-9.43]; P = .007). The appearance of a new symptomatic meniscal tear was the strongest significant predictor of high-grade PS at follow-up (OR = 4.31 [95% CI, 2.31-8.06]; P < .001). No significant correlation was observed between the addition of LET and the presence of high-grade PS at follow-up.
Conclusion: In the current study, 1 in 4 patients with high-grade PS before ACLR with or without LET was at risk of residual rotatory knee laxity at mean 44-month follow-up, regardless of the technique used. Repairing a pre-existing meniscal lesion was more effective than performing LET to decrease the presence of a high-grade PS at follow-up.
Keywords: anterior cruciate ligament reconstruction; lateral extra-articular tenodesis; meniscal tear; pivot shift; rotational laxity.
© The Author(s) 2021.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: S.P. has received consulting fees from Zimmer Biomet. C.S. has received consulting fees from Zimmer Biomet and Smith & Nephew. N.P. has received consulting fees from Zimmer Biomet and Smith & Nephew. M.O. has received consulting fees from Arthrex, Stryker, and Newclip. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Balazs GC, Greditzer HG, Wang D, et al. Non-treatment of stable ramp lesions does not degrade clinical outcomes in the setting of primary ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2020;28(11):3576–3586. - PubMed
-
- Burnett QM, Fowler PJ. Reconstruction of the anterior cruciate ligament: historical overview. Orthop Clin North Am. 1985;16(1):143–157. - PubMed
-
- Cavaignac E, Marot V, Faruch M, et al. Hamstring graft incorporation according to the length of the graft inside tunnels. Am J Sports Med. 2018;46(2):348–356. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
