

Prognostic utility of pretreatment neutrophil-lymphocyte ratio in survival outcomes in localized non-small cell lung cancer patients treated with stereotactic body radiotherapy: Selection of an ideal clinical cutoff point
- PMID: 33997320
- PMCID: PMC8089768
- DOI: 10.1016/j.ctro.2021.03.010
Prognostic utility of pretreatment neutrophil-lymphocyte ratio in survival outcomes in localized non-small cell lung cancer patients treated with stereotactic body radiotherapy: Selection of an ideal clinical cutoff point
Abstract
Background and purpose: Neutrophil-lymphocyte ratio (NLR) has been associated with overall survival (OS) in non-small cell lung cancer (NSCLC). We aimed to assess the utility of NLR as a predictor of lung cancer-specific survival (LCS) and identify an optimal, pretreatment cutoff point in patients with localized NSCLC treated with stereotactic body radiotherapy (SBRT) within the Veterans Affairs' (VA) national database.
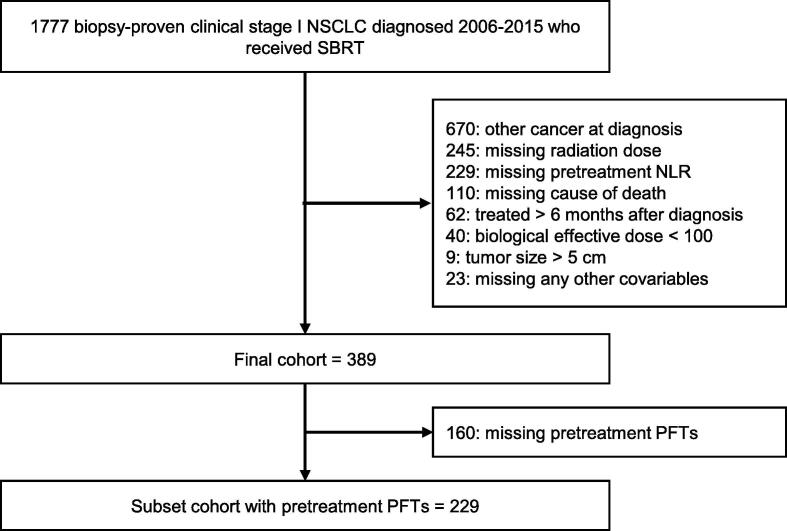
Materials and methods: In the VA database, we identified patients with biopsy-proven, clinical stage I NSCLC treated with SBRT between 2006 and 2015. Cutoff points for NLR were calculated using Contal/O'Quigley's and Cox Wald methods. Primary outcomes of OS, LCS, and non-lung cancer survival (NCS) were evaluated in Cox and Fine-Gray models.
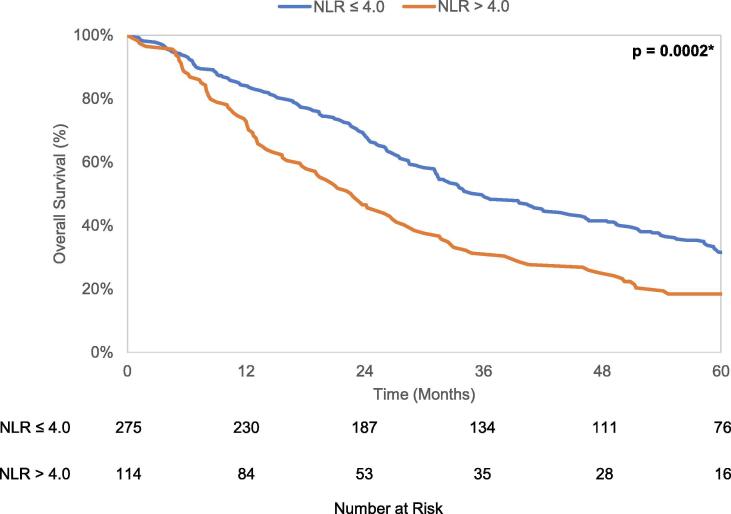
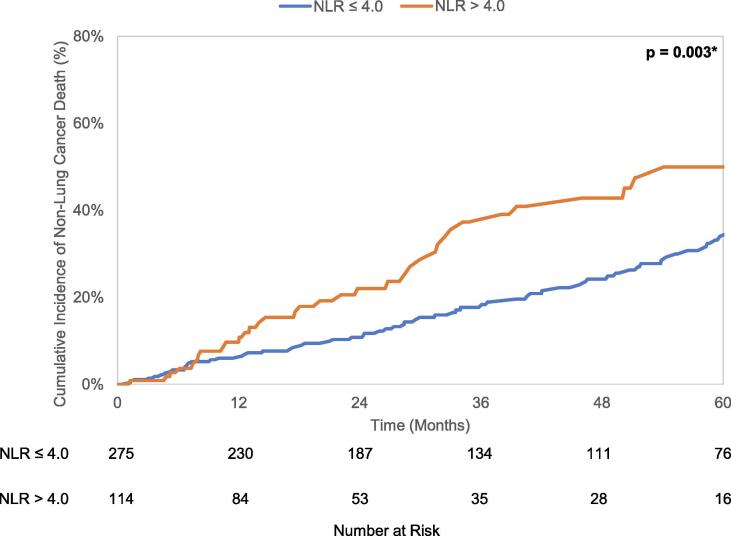
Results: In 389 patients, optimal NLR cutoff was identified as 4.0. In multivariable models, NLR > 4.0 was associated with decreased OS (HR 1.44, p = 0.01) and NCS (HR 1.68, p = 0.01) but not with LCS (HR 1.32, p = 0.09). In a subset analysis of 229 patients with pulmonary function tests, NLR > 4.0 remained associated with worse OS (HR 1.51, p = 0.02) and NCS (HR 2.18, p = 0.01) while the association with LCS decreased further (HR 1.22, p = 0.39).
Conclusion: NLR was associated with worse OS in patients with localized NSCLC treated with SBRT; however, NLR was only associated with NCS and not with LCS. Pretreatment NLR, with a cutoff of 4.0, offers potential as a marker of competing mortality risk which can aid in risk stratification in this typically frail and comorbid population. Further studies are needed to validate pretreatment NLR as a clinical tool in this setting.
Keywords: LCS, lung cancer-specific survival; NCS, non-lung cancer survival; NLR, Neutrophil-lymphocyte ratio; NSCLC, non-small cell lung cancer; Neutrophil-lymphocyte ratio; Non-small cell lung cancer; OS, overall survival; Prognostic factors; SBRT, stereotactic body radiotherapy; Stereotactic body radiotherapy; VA, Veterans Affairs; Veterans affairs (U.S.).
© 2021 Published by Elsevier B.V. on behalf of European Society for Radiotherapy and Oncology.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

Similar articles
-
Prognostic Utility of Pretreatment Neutrophil-Lymphocyte Ratio in Advanced Larynx Cancer.Biomark Insights. 2021 Oct 11;16:11772719211049848. doi: 10.1177/11772719211049848. eCollection 2021. Biomark Insights. 2021. PMID: 34658619 Free PMC article.
-
Association of neutrophil-lymphocyte ratio with survival in peripheral early-stage non-small cell lung cancer after stereotactic body radiation therapy.BMC Cancer. 2023 Mar 18;23(1):254. doi: 10.1186/s12885-023-10719-3. BMC Cancer. 2023. PMID: 36932396 Free PMC article.
-
Post-radiation neutrophil-to-lymphocyte ratio is a prognostic marker in patients with localized pancreatic adenocarcinoma treated with anti-PD-1 antibody and stereotactic body radiation therapy.Radiat Oncol J. 2022 Jun;40(2):111-119. doi: 10.3857/roj.2021.01060. Epub 2022 May 20. Radiat Oncol J. 2022. PMID: 35796114 Free PMC article.
-
Systemic Inflammatory Markers of Survival in Epidermal Growth Factor-Mutated Non-Small-Cell Lung Cancer: Single-Institution Analysis, Systematic Review, and Meta-analysis.Clin Lung Cancer. 2021 Sep;22(5):390-407. doi: 10.1016/j.cllc.2021.01.002. Epub 2021 Jan 10. Clin Lung Cancer. 2021. PMID: 33582072
-
Prognostic significance of the neutrophil to lymphocyte ratio in patients with non-small cell lung cancer: a systemic review and meta-analysis.Int J Clin Exp Med. 2015 Mar 15;8(3):3098-106. eCollection 2015. Int J Clin Exp Med. 2015. PMID: 26064198 Free PMC article. Review.
Cited by
-
Developing a clinical-radiomic prediction model for 3-year cancer-specific survival in lung cancer patients treated with stereotactic body radiation therapy.J Cancer Res Clin Oncol. 2024 Jan 26;150(2):34. doi: 10.1007/s00432-023-05536-x. J Cancer Res Clin Oncol. 2024. PMID: 38277078 Free PMC article.
-
External validation of radiobiological models for local control prediction in lung cancer patients treated with stereotactic body radiation therapy.Front Oncol. 2025 Jan 10;14:1431140. doi: 10.3389/fonc.2024.1431140. eCollection 2024. Front Oncol. 2025. PMID: 39902122 Free PMC article.
-
Incorporating the inflammation-related parameters enhances the performance of the nomogram for predicting local control in lung cancer patients treated with stereotactic body radiation therapy.J Cancer Res Clin Oncol. 2024 May 29;150(5):284. doi: 10.1007/s00432-024-05811-5. J Cancer Res Clin Oncol. 2024. PMID: 38811379 Free PMC article.
-
Impact of Pre-Treatment NLR and Other Hematologic Biomarkers on the Outcomes of Early-Stage Non-Small-Cell Lung Cancer Treated with Stereotactic Body Radiation Therapy.Curr Oncol. 2022 Jan 4;29(1):193-208. doi: 10.3390/curroncol29010019. Curr Oncol. 2022. PMID: 35049693 Free PMC article.
-
Development and validation of a nomogram for local control prediction in lung cancer patients treated with stereotactic body radiation therapy based on clinical, dosimetric, and inflammation-related parameters.BMC Pulm Med. 2025 Jul 10;25(1):332. doi: 10.1186/s12890-025-03800-z. BMC Pulm Med. 2025. PMID: 40634878 Free PMC article.
References
-
- Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2016, National Cancer Institute. Bethesda, MD, https://seer.cancer.gov/csr/1975_2016/, based on November 2018 SEER data submission, posted to the SEER web site, April 2019.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
