

Use of Post-Acute Care Services and Readmissions After Acute Myocardial Infarction Complicated by Cardiac Arrest and Cardiogenic Shock
- PMID: 33997631
- PMCID: PMC8105498
- DOI: 10.1016/j.mayocpiqo.2020.12.006
Use of Post-Acute Care Services and Readmissions After Acute Myocardial Infarction Complicated by Cardiac Arrest and Cardiogenic Shock
Abstract
Objective: To evaluate post-acute care utilization and readmissions after cardiac arrest (CA) and cardiogenic shock (CS) complicating acute myocardial infarction (AMI).
Methods: With use of an administrative claims database, AMI patients from January 1, 2010, to May 31, 2018, were stratified into CA+CS, CA only, CS only, and AMI alone. Outcomes included 90-day post-acute care (inpatient rehabilitation or skilled nursing facility) utilization and 1-year emergency department visits and readmissions.
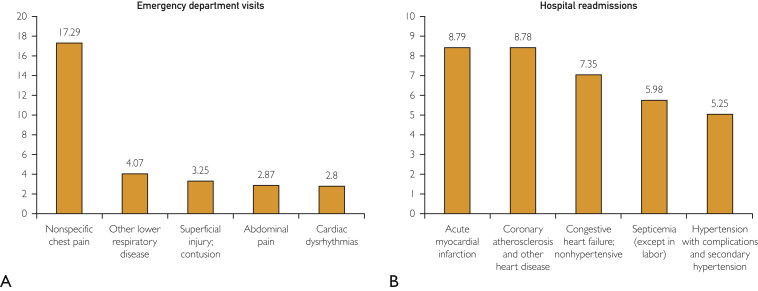
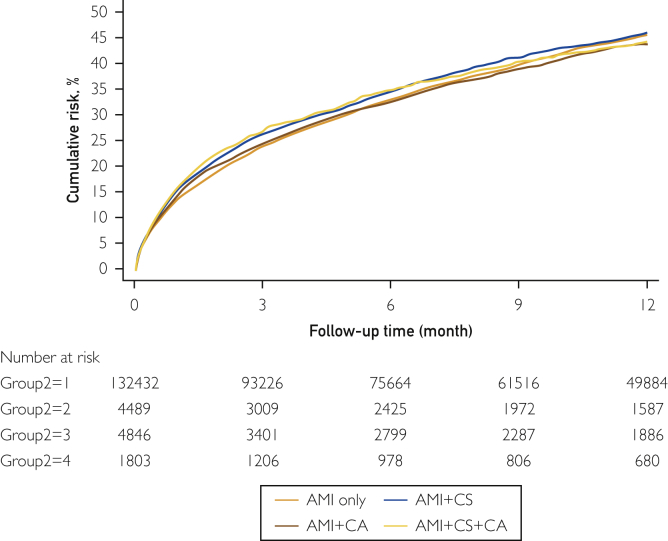
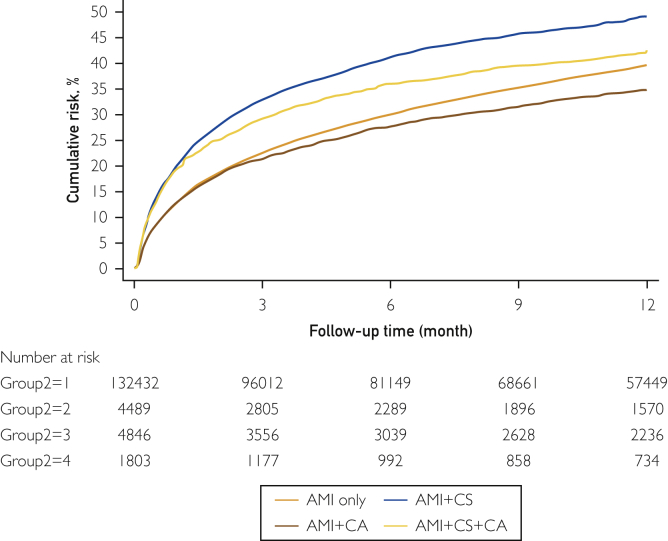
Results: Of 163,071 AMI patients, CA+CS, CA only, and CS only were noted in 3965 (2.4%), 8221 (5.0%), and 6559 (4.0%), respectively. In-hospital mortality was noted in 10,686 (6.6%) patients: CA+CS, 1935 (48.8%); CA only, 2948 (35.9%); CS only, 1578 (24.1%); and AMI alone, 4225 (2.9%) (P<.001). Among survivors, post-acute care services were used in 67,799 (44.5%), with higher use in the CS+CA cohort (1310 [64.6%]; hazard ratio [HR], 1.19; 95% CI, 1.06 to 1.33; P=.003) and CA cohort (2738 [51.9%]; HR, 1.27; 95% CI, 1.20 to 1.35; P<.001) but not in the CS cohort (3048 [61.2%]; HR, 1.03; 95% CI, 0.97 to 1.11; P=.35) compared with the AMI cohort (60,703 [43.3%]). Compared with the AMI cohort (48,990 [35.0%]), patients with CS only (2,085 [41.9%]; HR, 1.16; 95% CI, 1.10 to 1.22; P<.001) but not those with CA+CS (724 [35.7%]; HR, 1.07; 95% CI, 0.98 to 1.17; P=.14) had higher rates of readmissions (P=.03). Readmissions were lower in those with CA (1,590 [30.2%]; HR, 0.94; 95% CI, 0.89 to 0.99). Repeated AMI, coronary artery disease, and heart failure were the most common readmission reasons. There were no differences for emergency department visits.
Conclusion: CA is associated with increased post-acute care use, whereas CS is associated with increased readmission risk in AMI survivors.
Keywords: AMI, acute myocardial infarction; CA, cardiac arrest; CS, cardiogenic shock; ED, emergency department; HR, hazard ratio; ICD-10-CM, International Classification of Diseases, Tenth Revision, Clinical Modification; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; MCS, mechanical circulatory support; PCI, percutaneous coronary intervention; SNF, skilled nursing facility.
© 2020 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc.
Figures
References
-
- Vallabhajosyula S., Dunlay S.M., Barsness G.W., Rihal C.S., Holmes D.R., Jr., Prasad A. Hospital-level disparities in the outcomes of acute myocardial infarction with cardiogenic shock. Am J Cardiol. 2019;124(4):491–498. - PubMed
-
- Vallabhajosyula S., Dunlay S.M., Prasad A., et al. Acute noncardiac organ failure in acute myocardial infarction with cardiogenic shock. J Am Coll Cardiol. 2019;73(14):1781–1791. - PubMed
-
- Vallabhajosyula S., Vallabhajosyula S., Bell M.R., et al. Early vs. delayed in-hospital cardiac arrest complicating ST-elevation myocardial infarction receiving primary percutaneous coronary intervention. Resuscitation. 2020;148:242–250. - PubMed
-
- Jentzer J.C., Clements C.M., Murphy J.G., Scott Wright R. Recent developments in the management of patients resuscitated from cardiac arrest. J Crit Care. 2017;39:97–107. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
