

Perigeniculate arachnoid cysts and CSF fistulae of the fallopian canal: Histopathologic correlates of a rare clinical entity
- PMID: 33997715
- PMCID: PMC8103539
- DOI: 10.1016/j.wjorl.2020.12.005
Perigeniculate arachnoid cysts and CSF fistulae of the fallopian canal: Histopathologic correlates of a rare clinical entity
Abstract
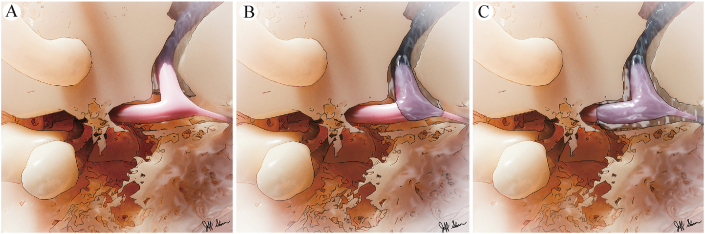
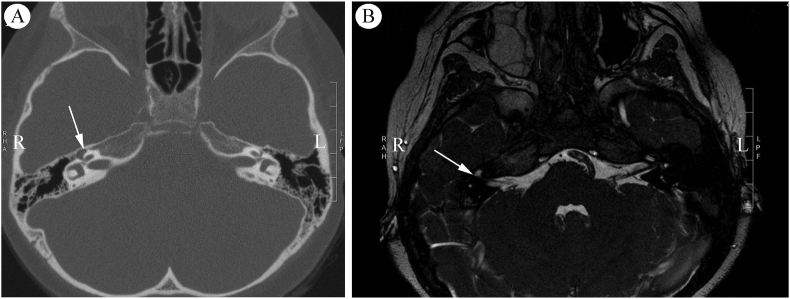
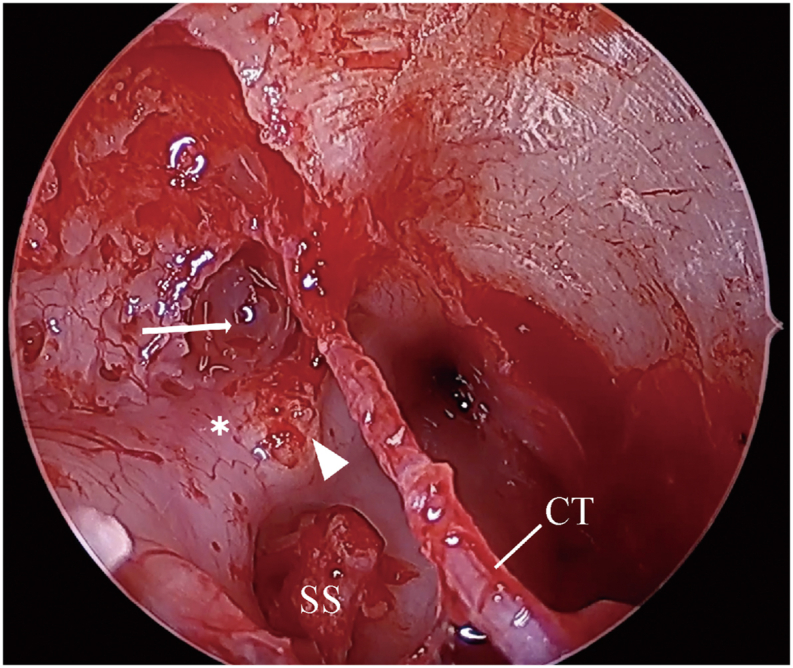
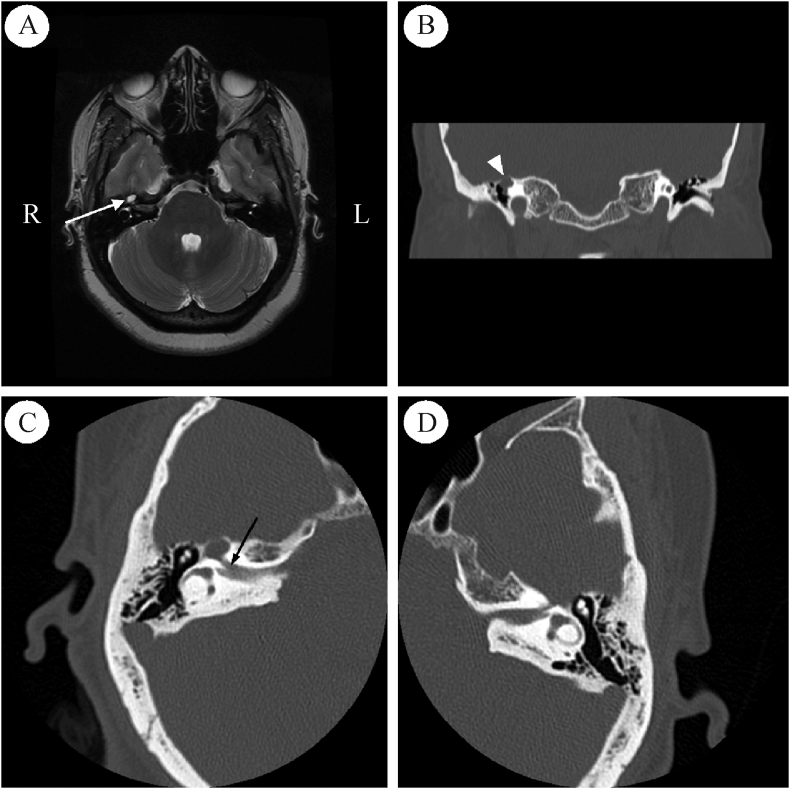
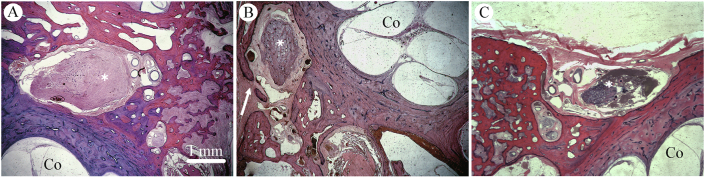
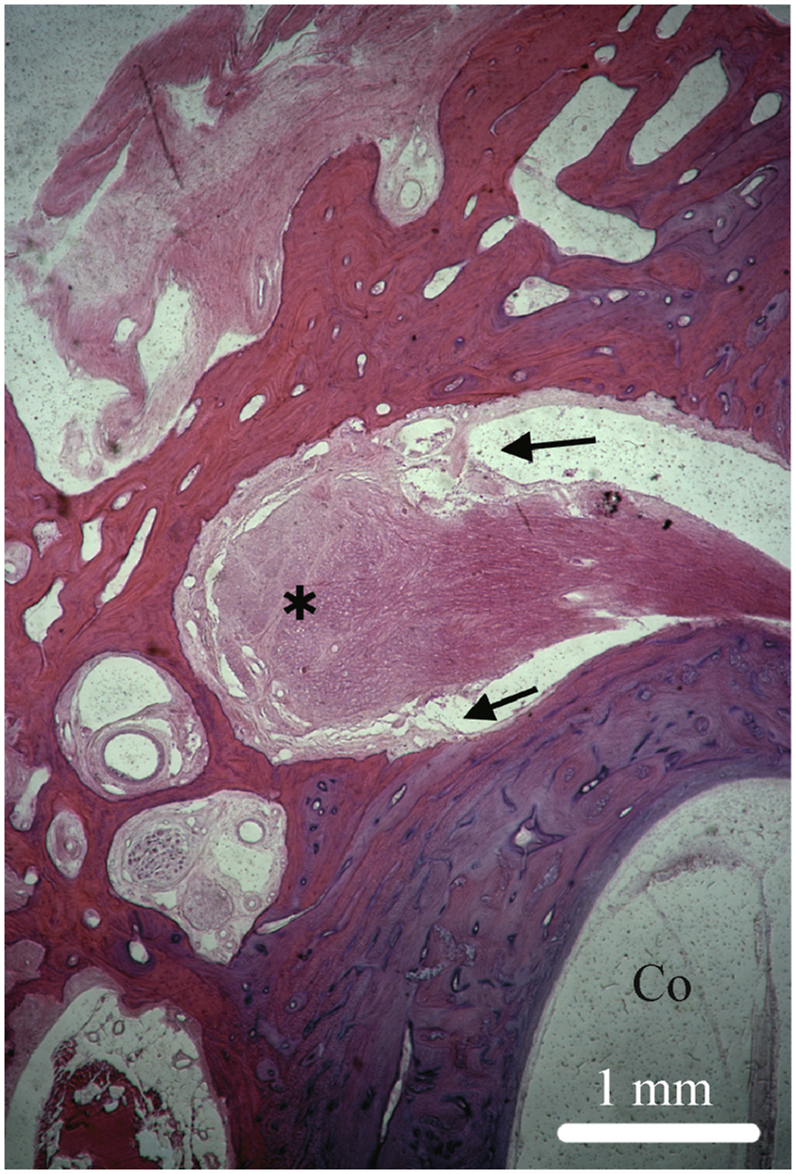
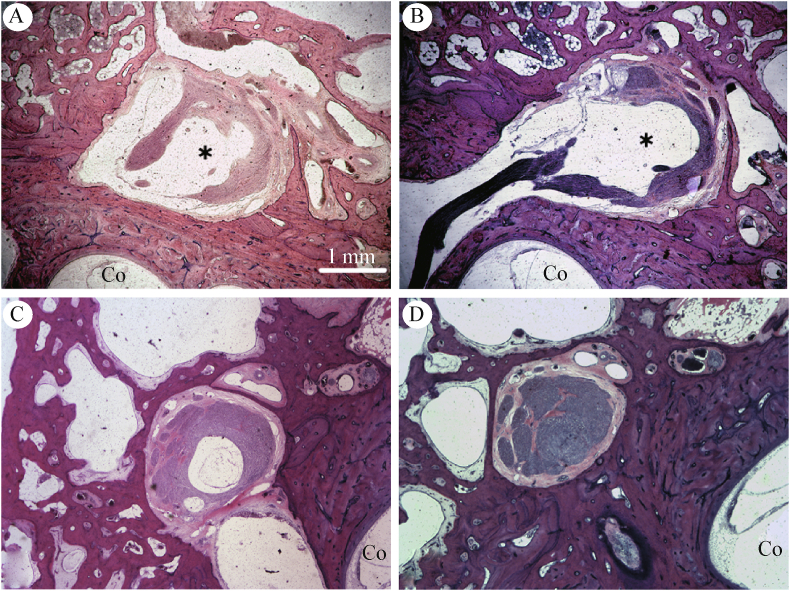
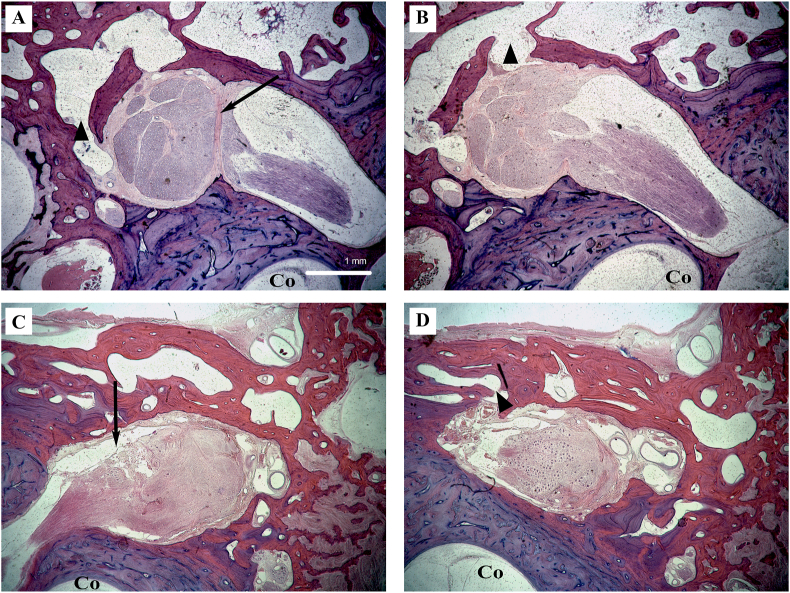
Cerebrospinal fluid (CSF) fistulae originating from the fallopian canal of the facial nerve is hypothesized to arise due to atypical patterns of subarachnoid space extension into the geniculate ganglion or more distal regions along the intratemporal course of the facial nerve, but its pathogenesis remains poorly understood. Although a rare etiology of CSF fistulae of the temporal bone, there are significant clinical ramifications due to the risk of recurrent meningitis, difficulty in identifying the anatomic location of the CSF leak, and technical challenges associated with surgical repair. We present three clinical cases of arachnoid cysts within the geniculate fossa with or without CSF fistulization and provide histopathologic correlates of this rare clinical phenomenon from a human temporal bone collection. The pediatric and adult patients presented suggest differential pathophysiologic mechanisms associated with CSF fistulae. Temporal bone histology reveals atypical patterns of subarachnoid space extension in the fallopian canal that may underlie arachnoid cyst formation and overt CSF leak from the geniculate region.
Keywords: Arachnoid cyst; Cerebrospinal fluid leak; Cerebrospinal fluid otorrhea; Facial nerve; Fallopian canal; Geniculate ganglion; Subarachnoid space.
© 2021 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Fallopian canal arachnoid cyst with acute facial nerve paralysis in children: a report of two cases and literature review.Front Neurol. 2023 Sep 4;14:1226404. doi: 10.3389/fneur.2023.1226404. eCollection 2023. Front Neurol. 2023. PMID: 37745664 Free PMC article.
-
Fallopian Canal Meningocele with Spontaneous Cerebrospinal Fluid Otorrhea: Case Report and Systematic Review of the Literature.World Neurosurg. 2019 Feb;122:e285-e290. doi: 10.1016/j.wneu.2018.10.021. Epub 2018 Oct 13. World Neurosurg. 2019. PMID: 30321684
-
Cerebrospinal fluid leak of the fallopian canal.Ear Nose Throat J. 2013 Mar;92(3):E20-3. Ear Nose Throat J. 2013. PMID: 23532657
-
Arachnoid cyst of the fallopian canal: a surgical challenge.Otol Neurotol. 2002 Jul;23(4):589-93. doi: 10.1097/00129492-200207000-00031. Otol Neurotol. 2002. PMID: 12170165
-
Challenges in the Management of Symptomatic Fallopian Canal Meningoceles: A Multicenter Case Series and Literature Review.Otol Neurotol. 2024 Apr 1;45(4):434-439. doi: 10.1097/MAO.0000000000004155. Otol Neurotol. 2024. PMID: 38478412 Review.
Cited by
-
Fallopian canal arachnoid cyst with acute facial nerve paralysis in children: a report of two cases and literature review.Front Neurol. 2023 Sep 4;14:1226404. doi: 10.3389/fneur.2023.1226404. eCollection 2023. Front Neurol. 2023. PMID: 37745664 Free PMC article.
References
-
- Proctor B., Nielsen E., Proctor C. Petrosquamosal suture and lamina. Otolaryngol Head Neck Surg. 1981;89:482–495. - PubMed
-
- Yew M., Dubbs B., Tong O. Arachnoid granulations of the temporal bone: a histologic study of dural and osseous penetration. Otol Neurotol. 2011;32:602–609. - PubMed
-
- Gacek R.R. Arachnoid granulation cerebrospinal fluid otorrhea. Ann Otol Rhinol Laryngol. 1990;99:854–862. - PubMed
-
- Åhrén C., Thulin C.A. Lethal intracranial complications following inflation in the external auditory canal in treatment of serous otitis media and due to defects in the petrous bone. Acta Otolaryngol. 1965;60:407–421.
-
- Lang D.V. Macroscopic bony deficiency of the tegmen tympani in adult temporal bones. J Laryngol Otol. 1983;97:685–688. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
