

Factors associated with deaths due to COVID-19 versus other causes: population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform
- PMID: 33997835
- PMCID: PMC8106239
- DOI: 10.1016/j.lanepe.2021.100109
Factors associated with deaths due to COVID-19 versus other causes: population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform
Abstract
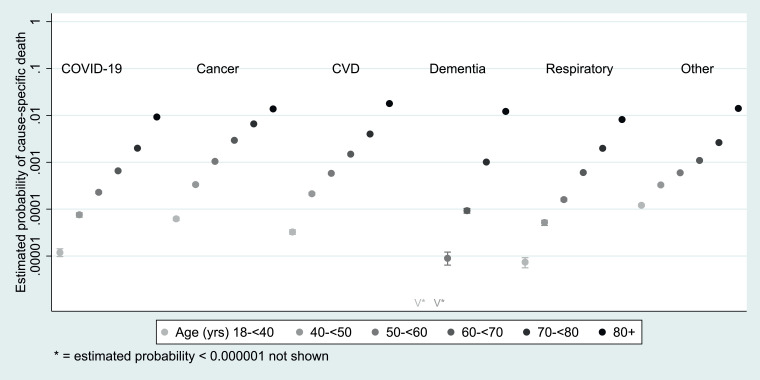
Background: Mortality from COVID-19 shows a strong relationship with age and pre-existing medical conditions, as does mortality from other causes. We aimed to investigate how specific factors are differentially associated with COVID-19 mortality as compared to mortality from causes other than COVID-19.
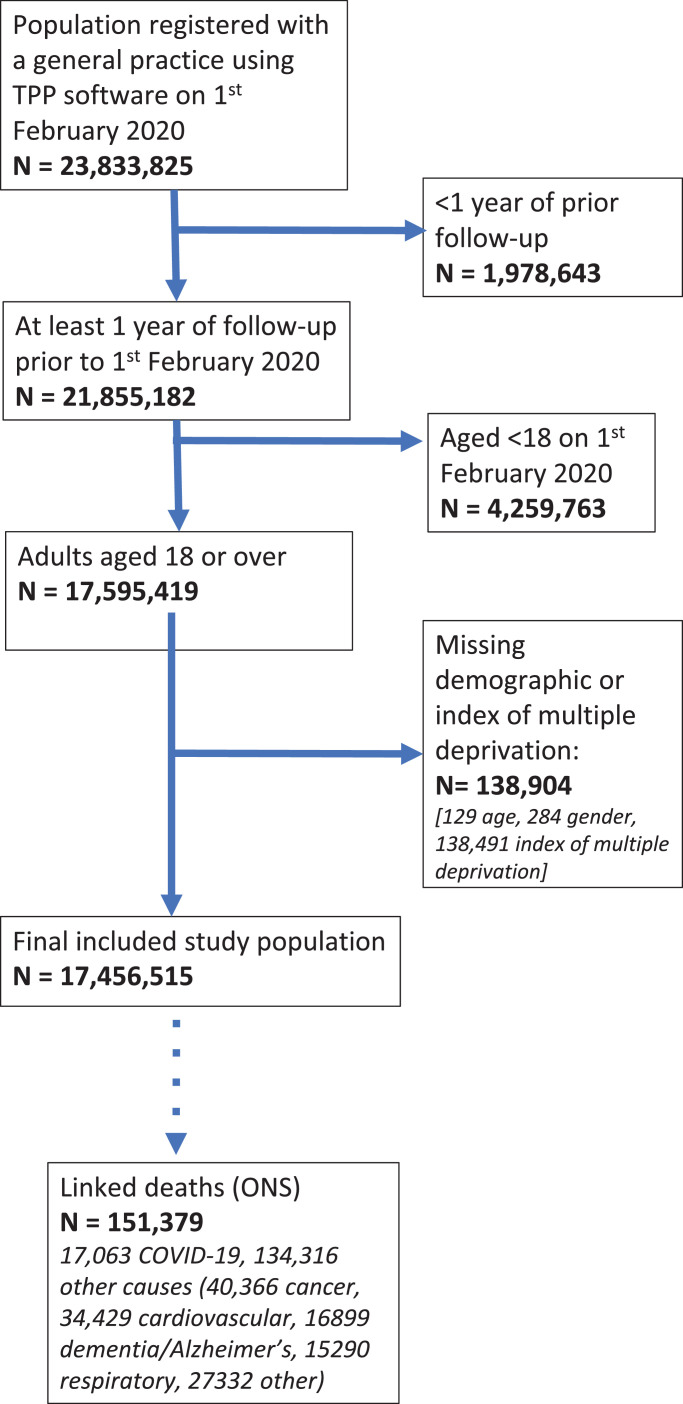
Methods: Working on behalf of NHS England, we carried out a cohort study within the OpenSAFELY platform. Primary care data from England were linked to national death registrations. We included all adults (aged ≥18 years) in the database on 1st February 2020 and with >1 year of continuous prior registration; the cut-off date for deaths was 9th November 2020. Associations between individual-level characteristics and COVID-19 and non-COVID deaths, classified according to the presence of a COVID-19 code as the underlying cause of death on the death certificate, were estimated by fitting age- and sex-adjusted logistic models for these two outcomes.
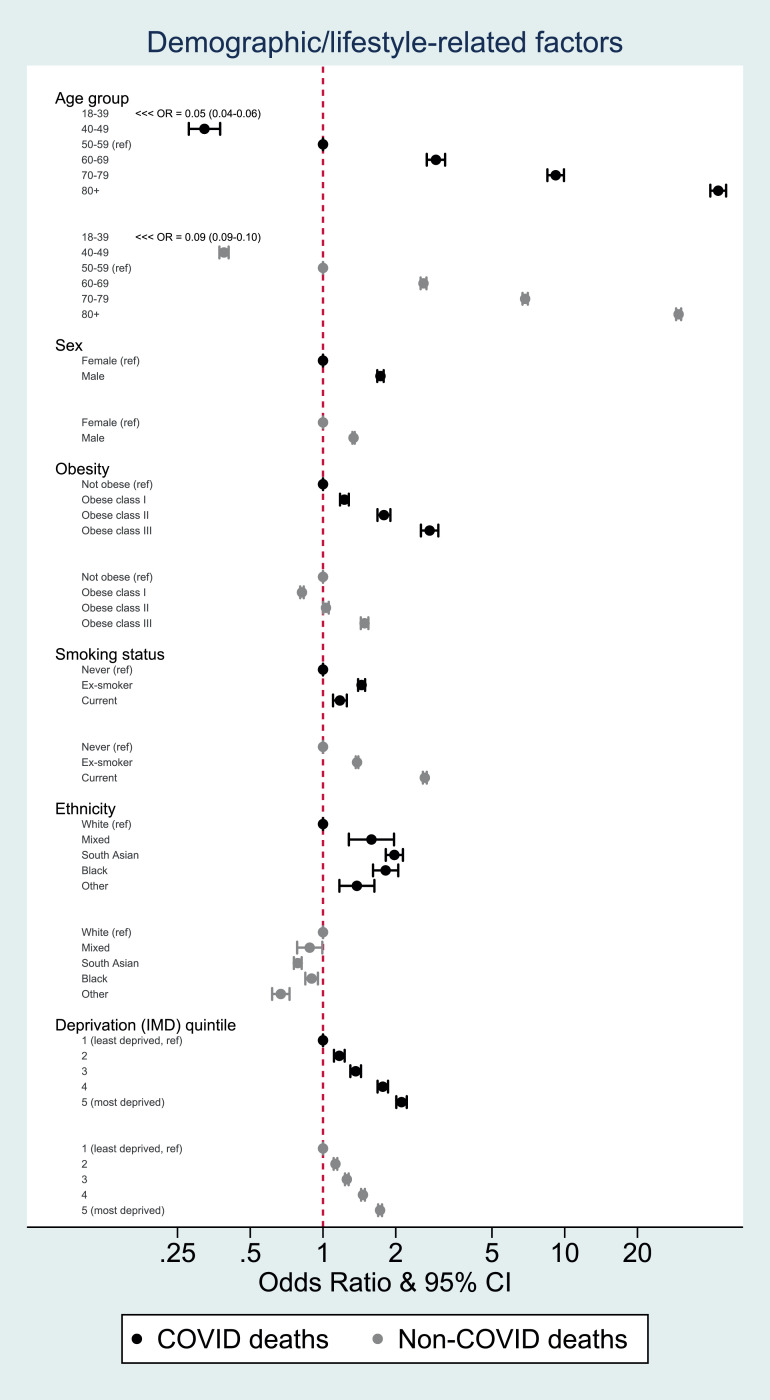
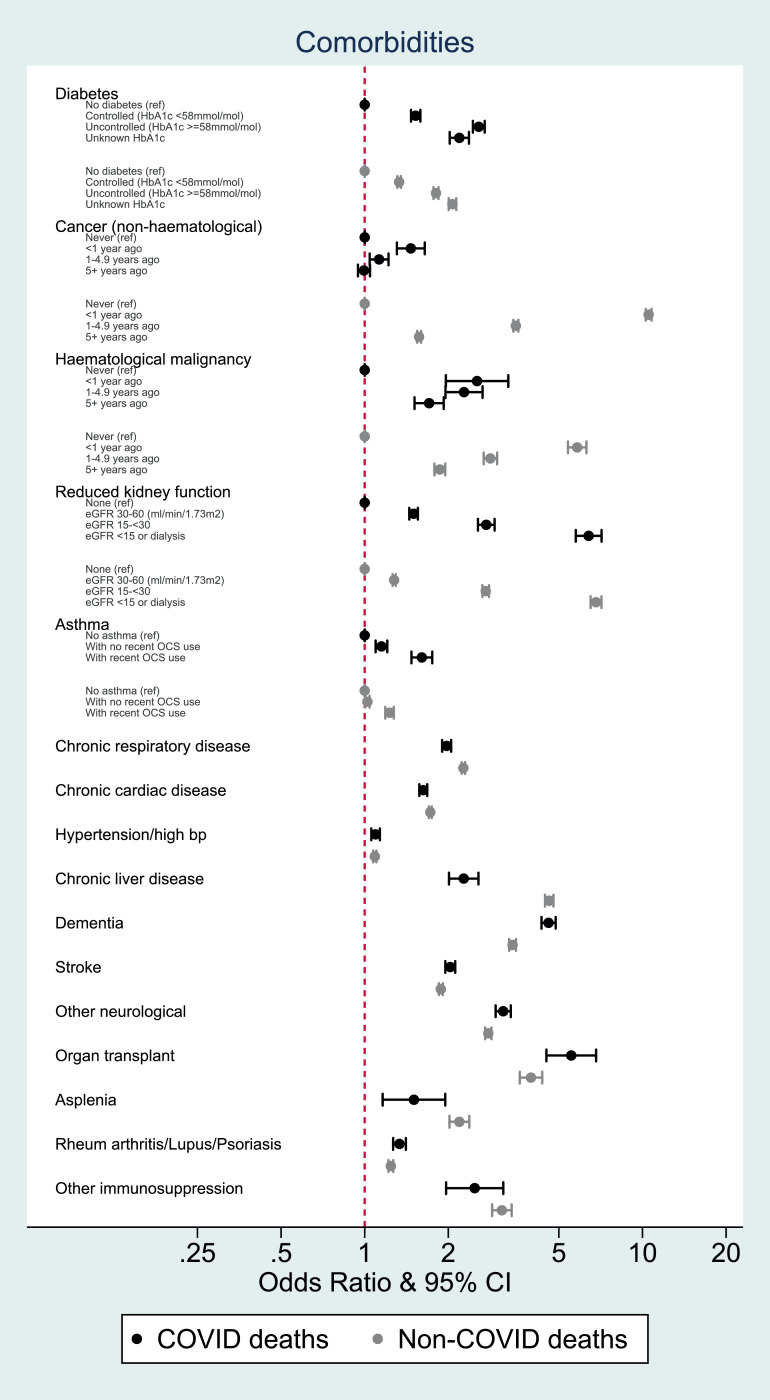
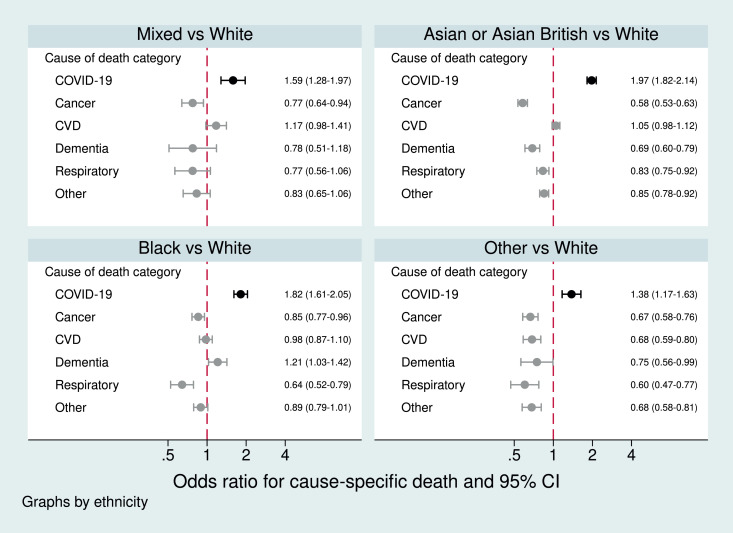
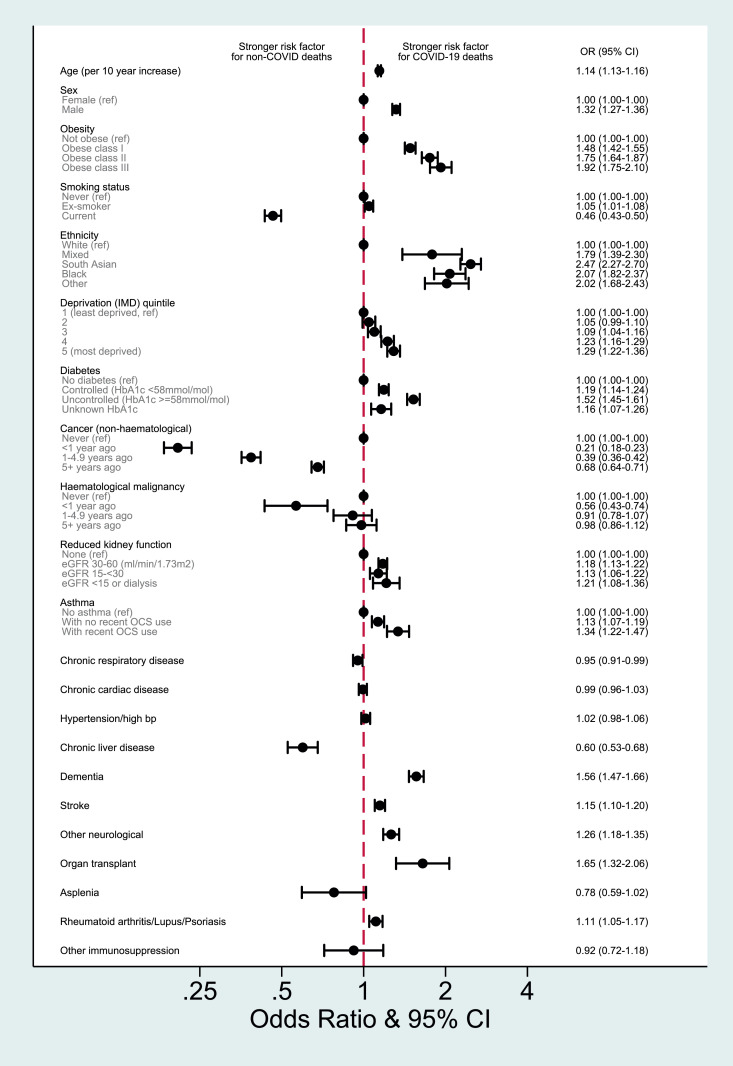
Findings: 17,456,515 individuals were included. 17,063 died from COVID-19 and 134,316 from other causes. Most factors associated with COVID-19 death were similarly associated with non-COVID death, but the magnitudes of association differed. Older age was more strongly associated with COVID-19 death than non-COVID death (e.g. ORs 40.7 [95% CI 37.7-43.8] and 29.6 [28.9-30.3] respectively for ≥80 vs 50-59 years), as was male sex, deprivation, obesity, and some comorbidities. Smoking, history of cancer and chronic liver disease had stronger associations with non-COVID than COVID-19 death. All non-white ethnic groups had higher odds than white of COVID-19 death (OR for Black: 2.20 [1.96-2.47], South Asian: 2.33 [2.16-2.52]), but lower odds than white of non-COVID death (Black: 0.88 [0.83-0.94], South Asian: 0.78 [0.75-0.81]).
Interpretation: Similar associations of most individual-level factors with COVID-19 and non-COVID death suggest that COVID-19 largely multiplies existing risks faced by patients, with some notable exceptions. Identifying the unique factors contributing to the excess COVID-19 mortality risk among non-white groups is a priority to inform efforts to reduce deaths from COVID-19.
Funding: Wellcome, Royal Society, National Institute for Health Research, National Institute for Health Research Oxford Biomedical Research Centre, UK Medical Research Council, Health Data Research UK.
Keywords: COVID-19; Epidemiology; Mortality.
© 2021 The Author(s).
Conflict of interest statement
TPP provided technical expertise and infrastructure within their data centre pro bono in the context of a national emergency. BG's work on better use of data in healthcare more broadly is currently funded in part by: NIHR Oxford Biomedical Research Centre, NIHR Applied Research Collaboration Oxford and Thames Valley, the Mohn-Westlake Foundation, NHS England, and the Health Foundation; all DataLab staff are supported by BG's grants on this work. LS reports grants from Wellcome, MRC, NIHR, UKRI, British Council, GSK, British Heart Foundation, and Diabetes UK outside this work. KB held a Sir Henry Dale fellowship (grant: 107731/Z/15/Z) jointly funded by Wellcome and the Royal Society and a Wellcome Senior Research Fellowship (grant: 220283/Z/20/Z) during this work. HIM is funded by the National Institute for Health Research (NIHR) Health Protection Research Unit in Immunisation, a partnership between Public Health England and LSHTM. EW holds grants from MRC. ID golds grants from NIHR and GSK. HF holds a UKRI fellowship. RME is funded by HDR UK (grant: MR/S003975/1) and MRC (grant: MC_PC 19065). The views expressed are those of the authors and not necessarily those of the NIHR, NHS England, Public Health England or the Department of Health and Social Care. Funders had no role in the study design, collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Figures
References
-
- European Centre for Disease Prevention and Control . 2020. COVID-19 situation update worldwide, as of 26 November 2020.https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases accessed 26 November 2020.
-
- Clift AK, Coupland CAC, Keogh RH, Diaz-Ordaz K, Williamson E, Harrison EM, Hayward A, Hemingway H, Horby P, Mehta N, Benger J, Khunti K, Spiegelhalter D, Sheikh A, Valabhji J, Lyons RA, Robson J, Semple MG, Kee F, Johnson P, Jebb S, Williams T, Hippisley-Cox J. Living risk prediction algorithm (QCOVID) for risk of hospital admission and mortality from coronavirus 19 in adults: national derivation and validation cohort study. BMJ. 2020;371:m3731. doi: 10.1136/bmj.m3731. - DOI - PMC - PubMed
-
- Mathur R, Rentsch CT, Morton C, Hulme WJ, Schultze A, MacKenna B, Eggo RM, Bhaskaran K, Wong AY, Williamson EJ, Forbes H, Wing K, McDonald HI, Bates C, Bacon S, Walker AJ, Evans D, Inglesby P, Mehrkar A, Curtis HJ, DeVito NJ, Croker R, Drysdale H, Cockburn J, Parry J, Hester F, Harper S, Douglas IJ, Tomlinson L, Evans S, Grieve R, Harrison D, Rowan K, Khunti K, Chaturvedi N, Smeeth L, Goldacre B. Ethnic differences in COVID-19 infection, hospitalisation, and mortality: an OpenSAFELY analysis of 17 million adults in England. Lancet (in press) 2021 - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
