

Intravenous Lignocaine-Fentanyl Versus Epidural Ropivacaine-Fentanyl for Postoperative Analgesia After Major Abdominal Oncosurgery: A Pilot Prospective Randomised Study
- PMID: 33997842
- PMCID: PMC8098735
- DOI: 10.5152/TJAR.2020.23326
Intravenous Lignocaine-Fentanyl Versus Epidural Ropivacaine-Fentanyl for Postoperative Analgesia After Major Abdominal Oncosurgery: A Pilot Prospective Randomised Study
Abstract
Objective: Epidural injection of local anaesthetics and intravenous opioid injection are two common analgesic strategies following major abdominal oncosurgery. However, epidural local anaesthetics may cause haemodynamic instability while opioid injection is associated with sedation and postoperative ileus. Intravenous lignocaine is also used for postoperative analgesia, and combined use of opioids plus lignocaine can reduce the doses and adverse effects of the individual drugs. This study therefore compared the analgesic efficacy of intravenous lignocaine-fentanyl (IV) to epidural ropivacaine-fentanyl (EPI) after major abdominal oncosurgery.
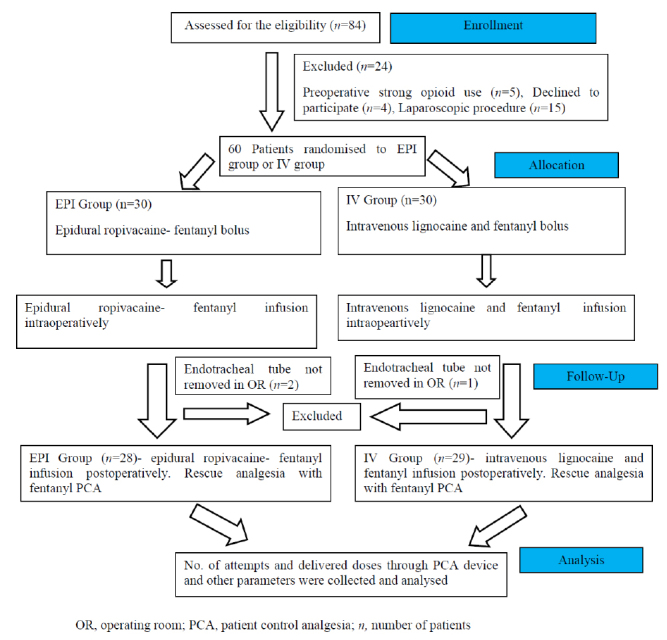
Methods: Sixty patients were randomised to IV and EPI groups. Patients in the IV group received preoperative intravenous bolus injections of lignocaine 1.5 mg kg-1 and fentanyl 0.5 μg kg-1, intraoperative infusions of lignocaine 1 mg kg-1 h-1 and fentanyl 0.5 μg kg-1 h-1, and postoperative infusions of lignocaine 0.5 mg kg-1 h-1 and fentanyl 0.25 μg kg-1 h-1. In the EPI group, patients received a 6-ml epidural bolus injection of ropivacaine 0.2% plus fentanyl 2 μg mL-1, intraoperative infusion of 5 mL·h-1 fentanyl and postoperative ropivacaine 0.1% plus fentanyl 1 μg mL-1 infusion at 5 mL h-1. All patients also received postoperative patient-controlled IV fentanyl as rescue analgesia. Patient-controlled fentanyl consumption was documented as the primary outcome for postoperative analgesic efficacy. Results were compared by Mann-Whitney U-test and Student's t-test using Statistical Package for Social Science (SPSS) software.
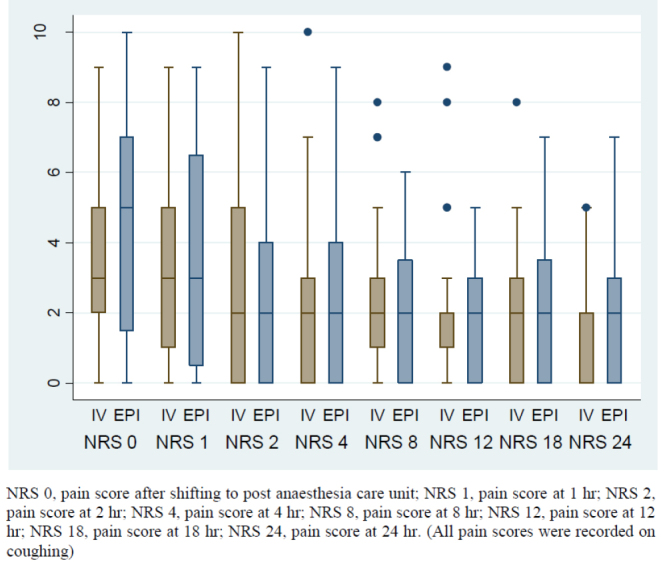
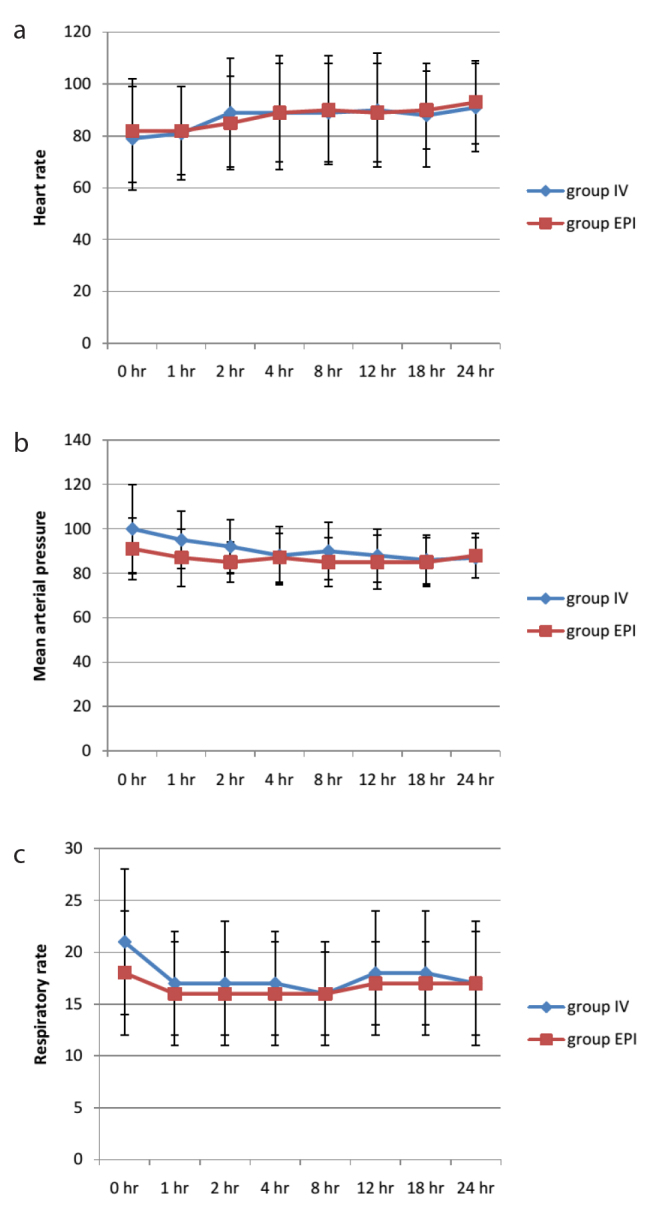
Results: Median (min-max) rescue fentanyl requirement in the first 24 h postsurgery was comparable between IV and EPI groups [780 (340-2520) μg vs. 820 (140-2260) μg; p=0.6], as was postoperative pain score (p>0.05). The incidence of intraoperative hypotension requiring bolus mephenteramine injection was significantly higher in the EPI group than the IV group (36% vs. 17%; p<0.001).
Conclusion: Intravenous lignocaine-fentanyl and epidural ropivacaine-fentanyl have comparable postoperative analgesic efficacies after major open abdominal oncosurgery.
Keywords: Analgesic technique; epidural local anaesthetic; fentanyl; intravenous lignocaine; postoperative analgesia.
© Copyright 2021 by Turkish Anaesthesiology and Intensive Care Society.
Conflict of interest statement
Conflict of interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
A comparison of two techniques of postoperative analgesia: lignocaine-fentanyl intravenous infusion and ropivacaine-fentanyl epidural infusion in patients undergoing cytoreductive cancer surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC)-prospective randomized control study.Langenbecks Arch Surg. 2023 Aug 24;408(1):330. doi: 10.1007/s00423-023-03078-x. Langenbecks Arch Surg. 2023. PMID: 37615724 Clinical Trial.
-
Patient-controlled epidural analgesia after Caesarean section: levobupivacaine 0.15% versus ropivacaine 0.15% alone or combined with fentanyl 2 µg/ml: a comparative study.Arch Med Sci. 2011 Aug;7(4):685-93. doi: 10.5114/aoms.2011.24140. Epub 2011 Sep 2. Arch Med Sci. 2011. PMID: 22291806 Free PMC article.
-
Comparative Evaluation of Ropivacaine and Fentanyl Versus Ropivacaine and Fentanyl with Clonidine for Postoperative Epidural Analgesia in Total Knee Replacement Surgery.J Clin Diagn Res. 2017 Sep;11(9):UC09-UC12. doi: 10.7860/JCDR/2017/25401.10615. Epub 2017 Sep 1. J Clin Diagn Res. 2017. PMID: 29207811 Free PMC article.
-
A Randomized Double Blinded Comparison of Epidural Infusion of Bupivacaine, Ropivacaine, Bupivacaine-Fentanyl, Ropivacaine-Fentanyl for Postoperative Pain Relief in Lower Limb Surgeries.J Clin Diagn Res. 2015 Sep;9(9):UC19-23. doi: 10.7860/JCDR/2015/15157.6459. Epub 2015 Sep 1. J Clin Diagn Res. 2015. PMID: 26500984 Free PMC article.
-
[Continuous peridural analgesia vs patient - controlled intravenous analgesia for pain therapy after thoracotomy].Anaesthesist. 2000 Jan;49(1):9-17. doi: 10.1007/s001010050003. Anaesthesist. 2000. PMID: 10662983 Review. German.
References
-
- Moraca RJ, Sheldon DG, Thirlby RC. The role of epidural anesthesia and analgesia in surgical practice. Ann Surg. 2003;238:663–73. doi: 10.1097/01.sla.0000094300.36689.ad. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources