

Diagnostic accuracy of a point-of-care aMMP-8 test in the discrimination of periodontal health and disease
- PMID: 33998040
- PMCID: PMC8362205
- DOI: 10.1111/jcpe.13485
Diagnostic accuracy of a point-of-care aMMP-8 test in the discrimination of periodontal health and disease
Abstract
Aim: To assess the diagnostic utility of an oral rinse active matrix metalloproteinase-8 (aMMP-8) point-of-care test (POCT) for differentiating periodontal health, gingivitis, as well as different stages and grades of periodontitis.
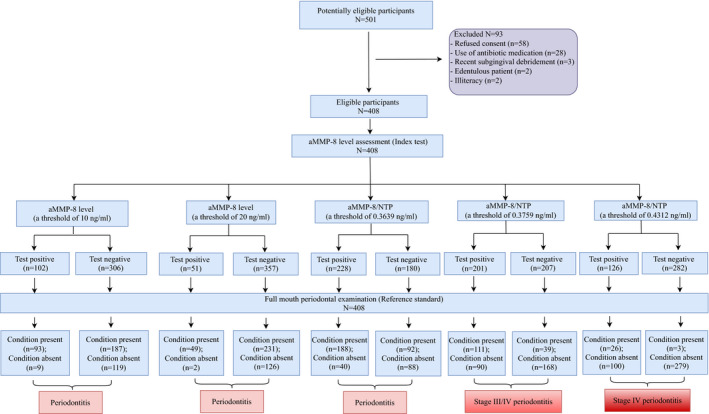
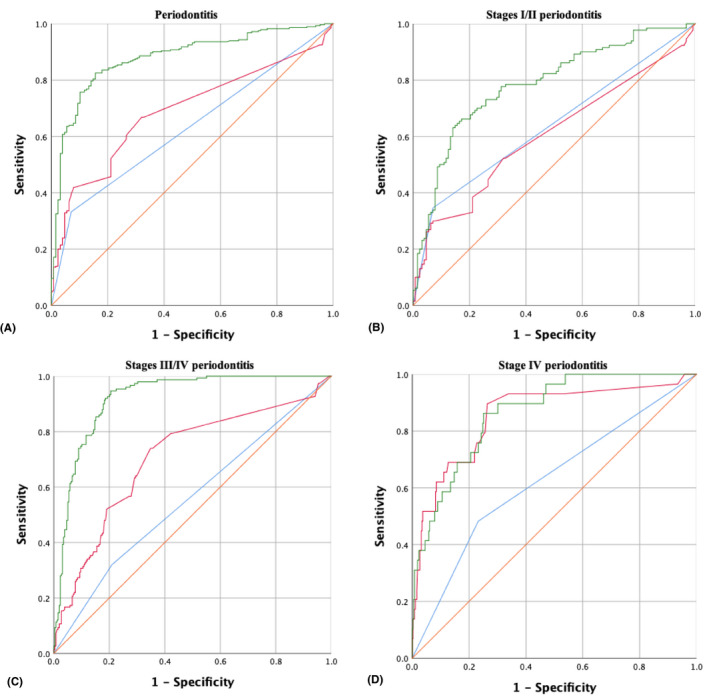
Materials & methods: The aMMP-8 index test was undertaken in 408 consecutive adults, followed by a full-mouth periodontal examination. The reference standard was the 2017 World Workshop classification of periodontal diseases. Sensitivity, specificity, and the area under the receiver operating characteristic curve (AUROC) were assessed.
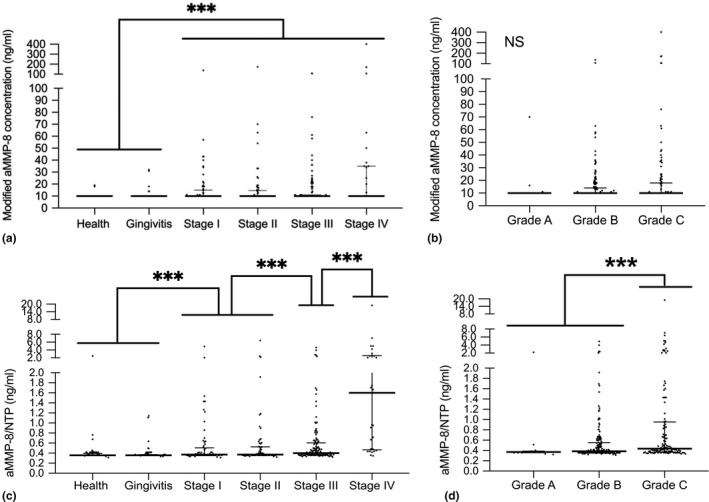
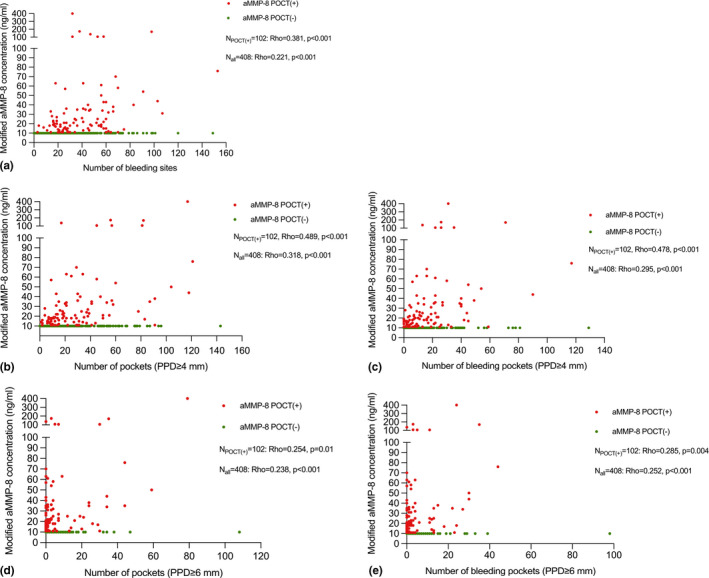
Results: 68.6% of the participants were diagnosed with periodontitis, including Stages I (15.9%), II (15.9%), III (29.7%) and IV (7.1%). A positive aMMP-8 POCT was associated with periodontitis after adjusting for age, gender, tobacco smoking and systemic diseases, while it was unable to differentiate among the stages/grades of periodontitis and between gingivitis/periodontal health. This test showed a sensitivity of 33.2% and a specificity of 93.0% for detecting periodontitis (threshold level >10 ng/ml). The levels of aMMP-8 adjusted by the number of teeth present (aMMP-8/NTP) performed better for periodontitis (sensitivity: 67.1%; specificity: 68.8%). Notably, aMMP-8/NTP were strongly predictive for Stage IV periodontitis (threshold level =0.4312 ng/ml) (sensitivity: 89.7%; specificity: 73.6%; and AUROC: 0.856). The test performance greatly improved in combination with age and smoking, with a sensitivity of 82.5%, a specificity of 84.4%, and an AUROC of 0.883.
Conclusion: This aMMP-8 POCT is able to detect periodontitis with better specificity than sensitivity across the spectrum of its severity. This test may be useful for periodontal screening in conjunction with subject characteristics and/or other sensitive screening tools. Further validation studies are needed.
Keywords: diagnosis; gingivitis; matrix metalloproteinase-8; periodontal health; periodontitis; point-of-care test; screening; sensitivity and specificity.
© 2021 The Authors. Journal of Clinical Periodontology published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors report no conflict of interest with this study.
Figures
Comment in
-
Authors' Response: "Diagnostic accuracy of a point-of-care aMMP-8 test in the discrimination of periodontal health and disease".J Clin Periodontol. 2021 Nov;48(11):1499-1500. doi: 10.1111/jcpe.13522. Epub 2021 Jul 29. J Clin Periodontol. 2021. PMID: 34265866 No abstract available.
-
On the accuracy, sensitivity, and grading of mouthrinse active matrix metalloproteinase-8 (aMMP-8) point-of-care testing (POCT).J Clin Periodontol. 2021 Nov;48(11):1495-1498. doi: 10.1111/jcpe.13521. Epub 2021 Aug 19. J Clin Periodontol. 2021. PMID: 34312914 No abstract available.
Similar articles
-
Diagnostic accuracy of active matrix metalloproteinase-8 point-of-care test for the discrimination of periodontal health status: Comparison of saliva and oral rinse samples.J Periodontal Res. 2022 Aug;57(4):768-779. doi: 10.1111/jre.12999. Epub 2022 May 16. J Periodontal Res. 2022. PMID: 35575900
-
Development of a machine learning multiclass screening tool for periodontal health status based on non-clinical parameters and salivary biomarkers.J Clin Periodontol. 2024 Dec;51(12):1547-1560. doi: 10.1111/jcpe.13856. Epub 2023 Sep 11. J Clin Periodontol. 2024. PMID: 37697491 Free PMC article.
-
Diagnostic Accuracy of a Point-Of-Care aMMP-8 Test for Discriminating Periodontal Health Status in Adults: Validation Trials and Updated Meta-Analysis.J Clin Periodontol. 2025 Apr;52(4):510-529. doi: 10.1111/jcpe.14119. Epub 2025 Jan 13. J Clin Periodontol. 2025. PMID: 39806539 Free PMC article.
-
Validation of a noninvasive aMMP-8 point-of-care diagnostic methodology in COVID-19 patients with periodontal disease.Clin Exp Dent Res. 2022 Aug;8(4):988-1001. doi: 10.1002/cre2.589. Epub 2022 Jul 11. Clin Exp Dent Res. 2022. PMID: 35818743 Free PMC article.
-
Diagnostic accuracy of salivary active matrix metalloproteinase (aMMP)-8 point-of-care test for detecting periodontitis in adults: A systematic review and meta-analysis.J Clin Periodontol. 2024 Aug;51(8):1093-1108. doi: 10.1111/jcpe.14000. Epub 2024 May 19. J Clin Periodontol. 2024. PMID: 38763168
Cited by
-
A Comparative Analysis of Treatment-Related Changes in the Diagnostic Biomarker Active Metalloproteinase-8 Levels in Patients with Periodontitis.Diagnostics (Basel). 2023 Feb 27;13(5):903. doi: 10.3390/diagnostics13050903. Diagnostics (Basel). 2023. PMID: 36900047 Free PMC article.
-
Correlations between different protein species of oral rinse MMP-8 and patient-related factors.Clin Exp Dent Res. 2023 Dec;9(6):1021-1033. doi: 10.1002/cre2.803. Epub 2023 Oct 25. Clin Exp Dent Res. 2023. PMID: 37877535 Free PMC article.
-
Active MMP-8 Quantitative Test as an Adjunctive Tool for Early Diagnosis of Periodontitis.Diagnostics (Basel). 2021 Aug 20;11(8):1503. doi: 10.3390/diagnostics11081503. Diagnostics (Basel). 2021. PMID: 34441437 Free PMC article.
-
Association between metabolic syndrome and salivary MMP-8, myeloperoxidase in periodontitis.Oral Dis. 2025 Jan;31(1):225-238. doi: 10.1111/odi.15014. Epub 2024 Jun 9. Oral Dis. 2025. PMID: 38852177 Free PMC article.
-
Prediabetes Associates with Matrix Metalloproteinase-8 Activation and Contributes to the Rapid Destruction of Periodontal Tissues.Eur J Dent. 2025 May;19(2):305-314. doi: 10.1055/s-0044-1788797. Epub 2024 Oct 1. Eur J Dent. 2025. PMID: 39353614 Free PMC article.
References
-
- Arias‐Bujanda, N., Regueira‐Iglesias, A., Balsa‐Castro, C., Nibali, L., Donos, N., & Tomas, I. (2020). Accuracy of single molecular biomarkers in saliva for the diagnosis of periodontitis: A systematic review and meta‐analysis. Journal of Clinical Periodontology, 47(1), 2–18. 10.1111/jcpe.13202 - DOI - PubMed
-
- Chapple, I. L. C., Mealey, B. L., Van Dyke, T. E., Bartold, P. M., Dommisch, H., Eickholz, P., Geisinger, M. L., Genco, R. J., Glogauer, M., Goldstein, M., Griffin, T. J., Holmstrup, P., Johnson, G. K., Kapila, Y., Lang, N. P., Meyle, J., Murakami, S., Plemons, J., Romito, G. A., … Yoshie, H. (2018). Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri‐Implant Diseases and Conditions. Journal of Clinical Periodontology, 45(Suppl 20), S68–S77. 10.1111/jcpe.12940 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
