

Neutrophil-to-lymphocyte ratio and outcomes in patients with new-onset or worsening heart failure with reduced and preserved ejection fraction
- PMID: 33998162
- PMCID: PMC8318449
- DOI: 10.1002/ehf2.13424
Neutrophil-to-lymphocyte ratio and outcomes in patients with new-onset or worsening heart failure with reduced and preserved ejection fraction
Erratum in
-
Correction to: 'Neutrophil-to-lymphocyte ratio and outcomes in patients with new-onset or worsening heart failure with reduced and preserved ejection fraction'.ESC Heart Fail. 2023 Jun;10(3):2145. doi: 10.1002/ehf2.14362. Epub 2023 Mar 31. ESC Heart Fail. 2023. PMID: 36999341 Free PMC article. No abstract available.
Abstract
Aims: Inflammation is thought to play a role in heart failure (HF) pathophysiology. Neutrophil-to-lymphocyte ratio (NLR) is a simple, routinely available measure of inflammation. Its relationship with other inflammatory biomarkers and its association with clinical outcomes in addition to other risk markers have not been comprehensively evaluated in HF patients.
Methods: We evaluated patients with worsening or new-onset HF from the BIOlogy Study to Tailored Treatment in Chronic Heart Failure (BIOSTAT-CHF) study who had available NLR at baseline. The primary outcome was time to all-cause mortality or HF hospitalization. Outcomes were validated in a separate HF population.
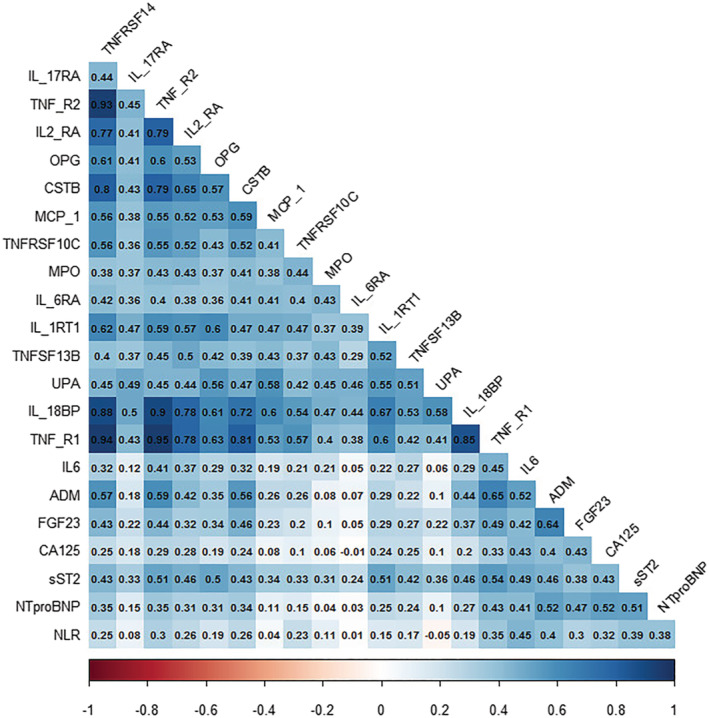
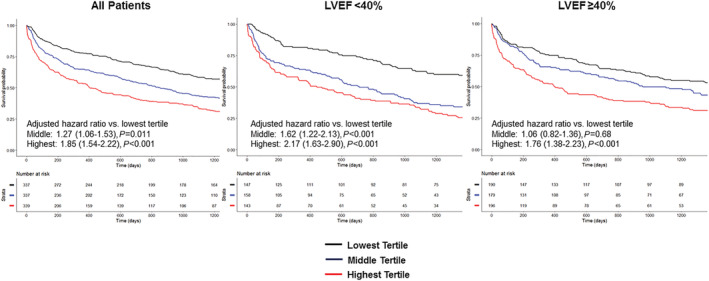
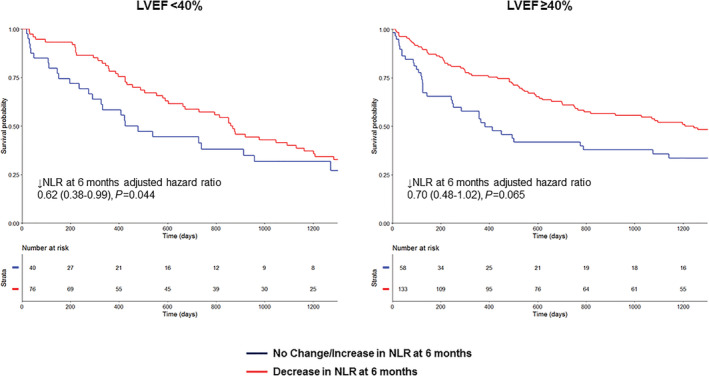
Results: 1622 patients were evaluated (including 523 ventricular ejection fraction [LVEF] < 40% and 662 LVEF ≥ 40%). NLR was significantly correlated with biomarkers related to inflammation as well as NT-proBNP. NLR was significantly associated with the primary outcome in patients irrespective of LVEF (hazard ratio [HR] 1.18 per standard deviation increase; 95% confidence interval [CI] 1.11-1.26, P < 0.001). Patients with NLR in the highest tertile had significantly worse outcome than those in the lowest independent of LVEF (<40%: HR 2.75; 95% CI 1.84-4.09, P < 0.001; LVEF ≥ 40%: HR 1.51; 95% CI 1.05-2.16, P = 0.026). When NLR was added to the BIOSTAT-CHF risk score, there were improvements in integrated discrimination index (IDI) and net reclassification index (NRI) for occurrence of the primary outcome (IDI + 0.009; 95% CI 0.00-0.019, P = 0.030; continuous NRI + 0.112, 95% CI 0.012-0.176, P = 0.040). Elevated NLR was similarly associated with adverse outcome in the validation cohort. Decrease in NLR at 6 months was associated with reduced incidence of the primary outcome (HR 0.75; 95% CI 0.57-0.98, P = 0.036).
Conclusions: Elevated NLR is significantly associated with elevated markers of inflammation in HF patients and is associated with worse outcome. Elevated NLR might potentially be useful in identifying high-risk HF patients and may represent a treatment target.
Keywords: Biomarkers; Heart failure; Inflammation; Neutrophil-to-lymphocyte ratio; Outcome.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
We report no specific conflict of interest related to this study. S.D.A. reports receiving fees from Bayer, Boehringer Ingelheim, Cardiac Dimension, Impulse Dynamics, Novartis, Servier, St. Jude Medical and Vifor Pharma and grant support from Abbott Vascular and Vifor Pharma. A.A.V. reports personal fees from Amgen, personal fees from cytokinetics, personal fees from Boehringer Ingelheim, personal fees from Vifor, grants and personal fees from Roche, personal fees from Novartis, personal fees from Servier, personal fees from AstraZeneca, personal fees from Bayer, personal fees from GSK, personal fees from Myokardia and personal fees from Merck, outside the submitted work. L.L.N. and D.J.V. report grants from EU FP7 Program during the conduct of the study. C.C.L. received fees and/or research grants from Novartis, AstraZeneca and MSD. M.M. received consulting or speaker fees from Amgen, AstraZeneca, Bayer, Novartis, Relypsa, Servier, Stealth Therapeutics, Trevena and Abbott Vascular. GF reports grants from EU; Lecture and /or Committee member fees in trials sponsored by Bayer, Boehringer Ingelheim, Amgen, Medtronic, Novartis, Servier outside this work. All other authors have nothing to declare.
Figures
References
-
- Levine B, Kalman J, Mayer L, Fillit HM, Packer M. Elevated circulating levels of tumor necrosis factor in severe chronic heart failure. N Engl J Med 1990; 323: 236–241. - PubMed
-
- Gullestad L, Ureland T, Vinge LE, Finsen A, Yndestad A, Aukrust P. Inflammatory cytokines in heart failure: mediators and markers. Cardiology 2012; 122: 23–35. - PubMed
-
- Deswal A, Petersen NJ, Feldman AM, Young JB, White BG, Mann DL. Cytokines and cytokine receptors in advanced heart failure: an analysis of the cytokine database from the vesnarinone trial (VEST). Circulation 2001; 103: 2055–2059. - PubMed
-
- Ferrari R, Bachetti T, Confortini R, Opasich C, Febo O, Corti A, Cassani G, Visioli O. Tumor necrosis factor soluble receptors in patients with various degrees of congestive heart failure. Circulation 1995; 92: 1479–1486. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
