

Racial differences in the treatment and outcomes for prostate cancer in Massachusetts
- PMID: 33999405
- PMCID: PMC9107927
- DOI: 10.1002/cncr.33564
Racial differences in the treatment and outcomes for prostate cancer in Massachusetts
Abstract
Background: Massachusetts is a northeastern state with universally mandated health insurance since 2006. Although Black men have generally worse prostate cancer outcomes, emerging data suggest that they may experience equivalent outcomes within a fully insured system. In this setting, the authors analyzed treatments and outcomes of non-Hispanic White and Black men in Massachusetts.
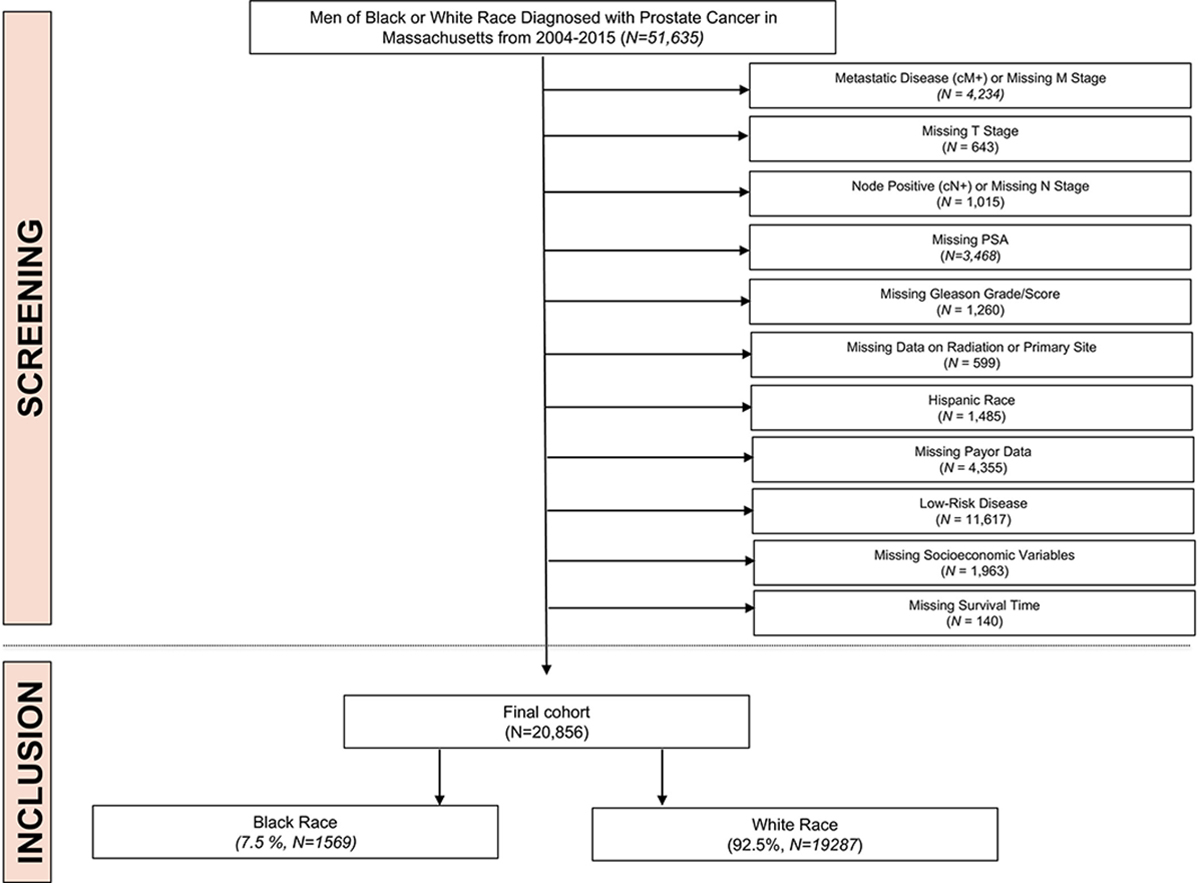
Methods: White and Black men who were 20 years old or older and had been diagnosed with localized intermediate- or high-risk nonmetastatic prostate cancer in 2004-2015 were identified in the Massachusetts Cancer Registry. Adjusted logistic regression models were used to assess predictors of definitive therapy. Adjusted and unadjusted survival models compared cancer-specific mortality. Interaction terms were then used to assess whether the effect of race varied between counties.
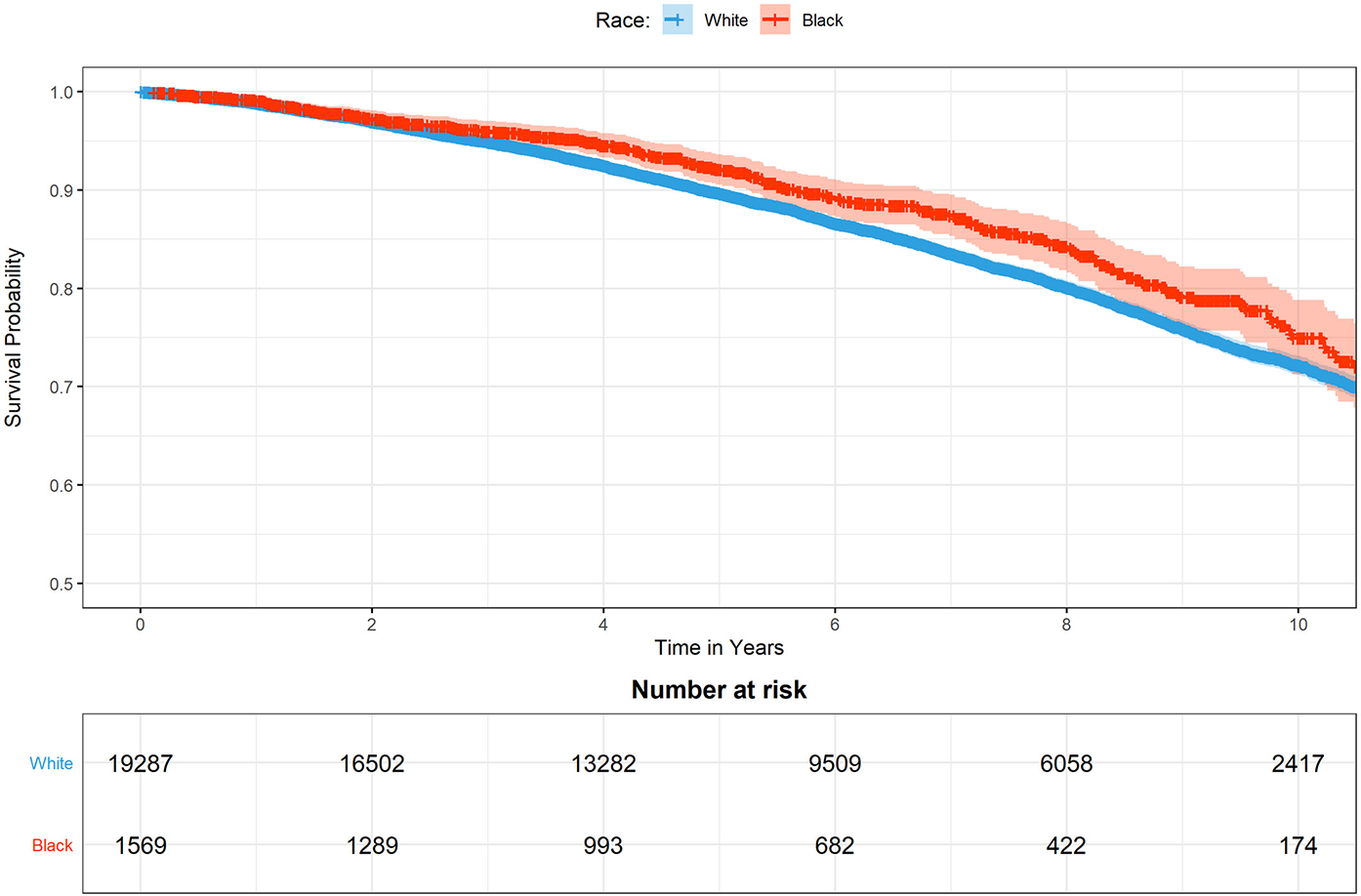
Results: A total of 20,856 men were identified. Of these, 19,287 (92.5%) were White. There were significant county-level differences in the odds of receiving definitive therapy and survival. Survival was worse for those with high-risk cancer (adjusted hazard ratio [HR], 1.50; 95% CI, 1.4-1.60) and those with public insurance (adjusted HR for Medicaid, 1.69; 95% CI, 1.38-2.07; adjusted HR for Medicare, 1.2; 95% CI, 1.14-1.35). Black men were less likely to receive definitive therapy (adjusted odds ratio, 0.78; 95% CI, 0.74-0.83) but had a 17% lower cancer-specific mortality (adjusted HR, 0.83; 95% CI, 0.7-0.99).
Conclusions: Despite lower odds of definitive treatment, Black men experience decreased cancer-specific mortality in comparison with White men in Massachusetts. These data support the growing body of research showing that Black men may achieve outcomes equivalent to or even better than those of White men within the context of a well-insured population.
Lay summary: There is a growing body of evidence showing that the excess risk of death among Black men with prostate cancer may be caused by disparities in access to care, with few or no disparities seen in universally insured health systems such as the Veterans Affairs and US Military Health System. Therefore, the authors sought to assess racial disparities in prostate cancer in Massachusetts, which was the earliest US state to mandate universal insurance coverage (in 2006). Despite lower odds of definitive treatment, Black men with prostate cancer experience reduced cancer-specific mortality in comparison with White men in Massachusetts. These data support the growing body of research showing that Black men may achieve outcomes equivalent to or even better than those of White men within the context of a well-insured population.
Keywords: prostate cancer; racial disparities; surgical outcomes.
© 2021 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
Speaker fees from Myovant; and stock options in Novavax. Quoc-Dien Trinh reports honoraria from Bayer, Janssen, and Astellas and research funding from Intuitive Surgical. The other authors made no disclosures.
Figures

References
-
- Brawley OW. Prostate cancer epidemiology in the United States. World J Urol. 2012;30:195–200. - PubMed
-
- Friedlander DF, Trinh QD, Krasnova A, et al. Racial disparity in delivering definitive therapy for intermediate/high-risk localized prostate cancer: the impact of facility features and socioeconomic characteristics. Eur Urol. 2018;73:445–451. - PubMed
-
- Trinh QD, Sun M, Sammon J, et al. Disparities in access to care at high-volume institutions for uro-oncologic procedures. Cancer. 2012;118:4421–4426. - PubMed
-
- Krimphove MJ, Cole AP, Fletcher SA, et al. Evaluation of the contribution of demographics, access to health care, treatment, and tumor characteristics to racial differences in survival of advanced prostate cancer. Prostate Cancer Prostatic Dis. 2019;22:125–136. - PubMed
-
- Aizer AA, Wilhite TJ, Chen MH, et al. Lack of reduction in racial disparities in cancer-specific mortality over a 20-year period. Cancer. 2014;120:1532–1539. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
