

Physical Rehabilitation for Older Patients Hospitalized for Heart Failure
- PMID: 33999544
- PMCID: PMC8353658
- DOI: 10.1056/NEJMoa2026141
Physical Rehabilitation for Older Patients Hospitalized for Heart Failure
Abstract
Background: Older patients who are hospitalized for acute decompensated heart failure have high rates of physical frailty, poor quality of life, delayed recovery, and frequent rehospitalizations. Interventions to address physical frailty in this population are not well established.
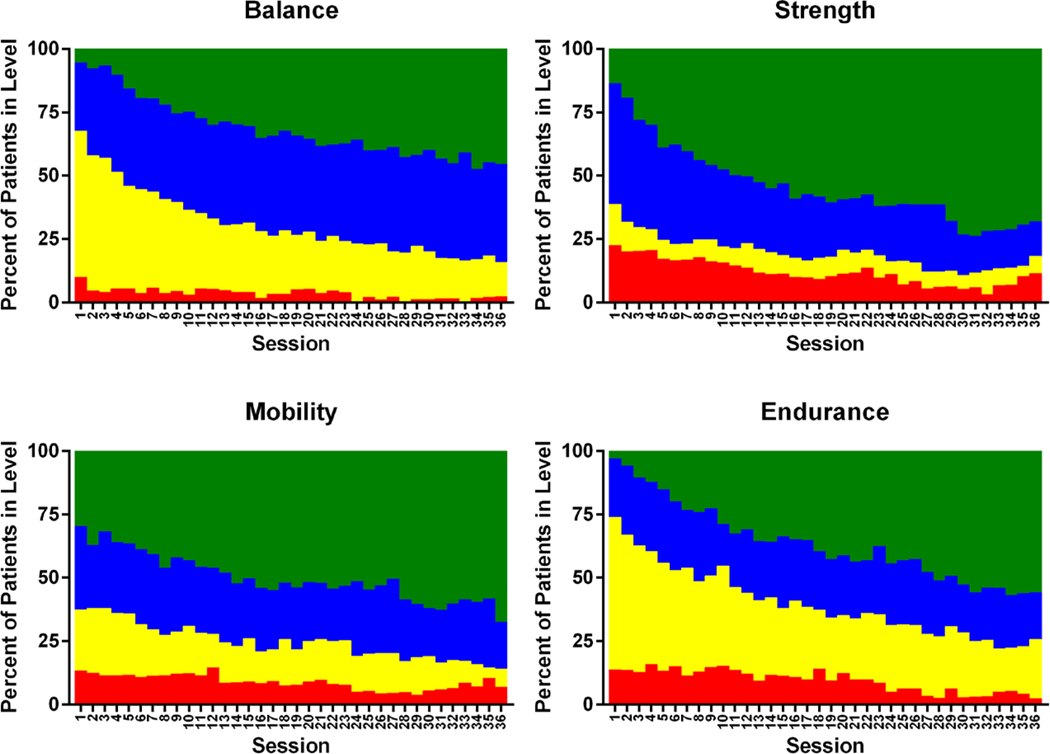
Methods: We conducted a multicenter, randomized, controlled trial to evaluate a transitional, tailored, progressive rehabilitation intervention that included four physical-function domains (strength, balance, mobility, and endurance). The intervention was initiated during, or early after, hospitalization for heart failure and was continued after discharge for 36 outpatient sessions. The primary outcome was the score on the Short Physical Performance Battery (total scores range from 0 to 12, with lower scores indicating more severe physical dysfunction) at 3 months. The secondary outcome was the 6-month rate of rehospitalization for any cause.
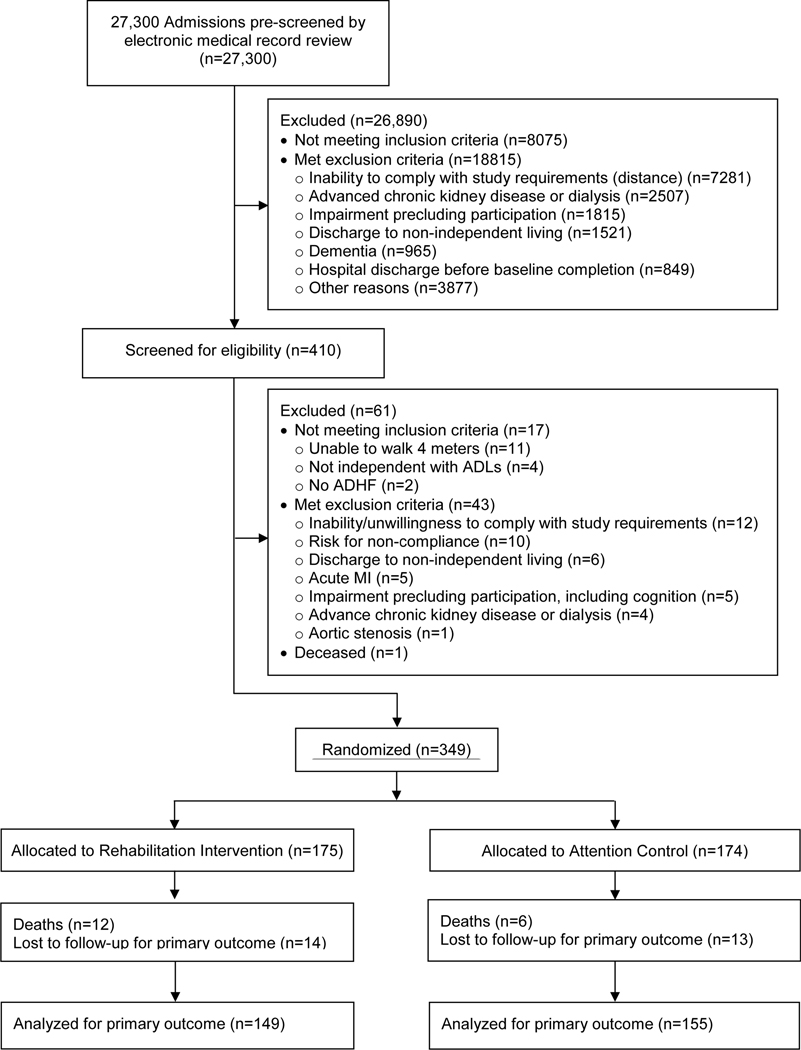
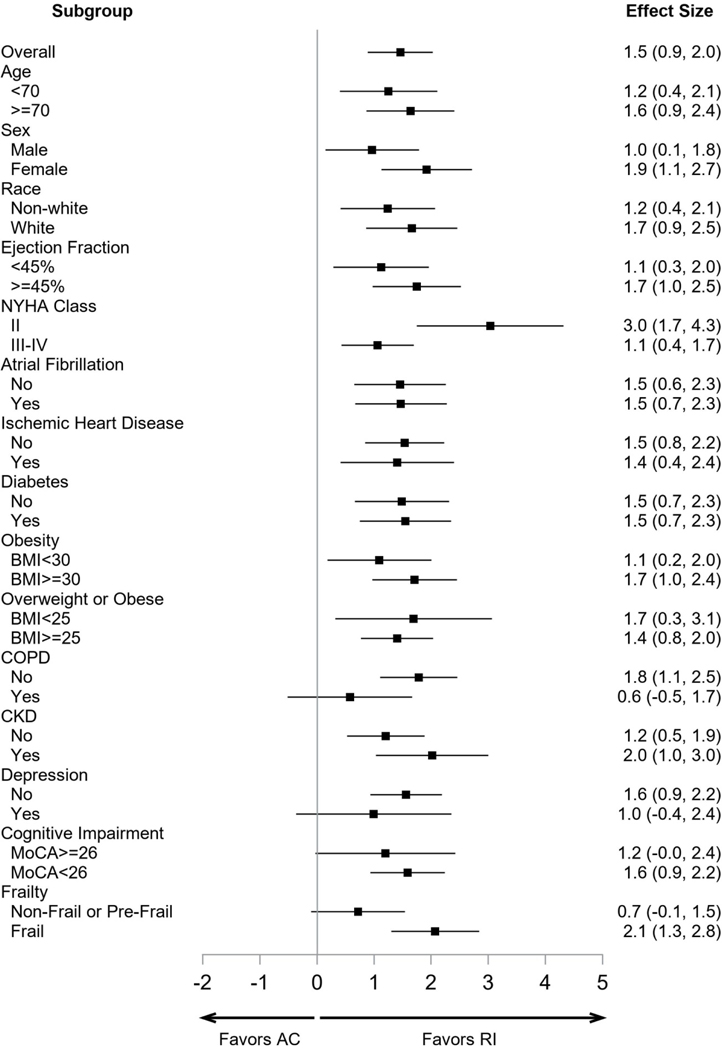
Results: A total of 349 patients underwent randomization; 175 were assigned to the rehabilitation intervention and 174 to usual care (control). At baseline, patients in each group had markedly impaired physical function, and 97% were frail or prefrail; the mean number of coexisting conditions was five in each group. Patient retention in the intervention group was 82%, and adherence to the intervention sessions was 67%. After adjustment for baseline Short Physical Performance Battery score and other baseline characteristics, the least-squares mean (±SE) score on the Short Physical Performance Battery at 3 months was 8.3±0.2 in the intervention group and 6.9±0.2 in the control group (mean between-group difference, 1.5; 95% confidence interval [CI], 0.9 to 2.0; P<0.001). At 6 months, the rates of rehospitalization for any cause were 1.18 in the intervention group and 1.28 in the control group (rate ratio, 0.93; 95% CI, 0.66 to 1.19). There were 21 deaths (15 from cardiovascular causes) in the intervention group and 16 deaths (8 from cardiovascular causes) in the control group. The rates of death from any cause were 0.13 and 0.10, respectively (rate ratio, 1.17; 95% CI, 0.61 to 2.27).
Conclusions: In a diverse population of older patients who were hospitalized for acute decompensated heart failure, an early, transitional, tailored, progressive rehabilitation intervention that included multiple physical-function domains resulted in greater improvement in physical function than usual care. (Funded by the National Institutes of Health and others; REHAB-HF ClinicalTrials.gov number, NCT02196038.).
Copyright © 2021 Massachusetts Medical Society.
Figures
Comment in
-
Exercise for Frail, Elderly Patients with Acute Heart Failure - A Strong Step Forward.N Engl J Med. 2021 Jul 15;385(3):276-277. doi: 10.1056/NEJMe2106140. Epub 2021 May 16. N Engl J Med. 2021. PMID: 33999546 No abstract available.
-
A tailored cardiac rehabilitation for patients with acute heart failure.Nat Rev Cardiol. 2021 Aug;18(8):544. doi: 10.1038/s41569-021-00580-x. Nat Rev Cardiol. 2021. PMID: 34045728 No abstract available.
-
Physical Rehabilitation in Patients with Heart Failure.N Engl J Med. 2021 Sep 30;385(14):1339-1340. doi: 10.1056/NEJMc2113494. N Engl J Med. 2021. PMID: 34587393 No abstract available.
-
Physical Rehabilitation in Patients with Heart Failure.N Engl J Med. 2021 Sep 30;385(14):1340. doi: 10.1056/NEJMc2113494. N Engl J Med. 2021. PMID: 34587394 No abstract available.
References
-
- Cheng R, Cox M, Neely M, et al.Outcomes in patients with heart failure with preserved, borderline, and reduced ejection fraction in the Medicare population. American Heart Journal 2014;168:731–30. - PubMed
-
- Fleg J Preventing Readmission After Hospitalization for Acute Heart Failure: A Quest Incompletely Fulfilled. JACC: Heart Failure 2018;6:153–5. - PubMed
-
- Alahdab M, Mansour I, Napan S, Stamos T. Six Minute Walk Test Predicts Long-Term All-Cause Mortality and Heart Failure Rehospitalization in African-American Patients Hospitalized With Acute Decompensated Heart Failure. J Card Fail 2009;15:130–5. - PubMed
-
- Chiarantini D, Volpato S, Sioulis F, et al.Lower extremity performance measures predict long-term prognosis in older patients hospitalized for heart failure. J Card Fail 2010;16:390–5. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous