

Clinical Trial
doi: 10.1161/CIRCEP.120.009747.
Epub 2021 May 17.
Durable Physiological Changes and Decreased Syncope Burden 12 Months After Unifocal Right-Sided Ablation Under Computed Tomographic Guidance in Patients With Neurally Mediated Syncope or Functional Sinus Node Dysfunction
Affiliations
- PMID: 33999698
- PMCID: PMC8208097
- DOI: 10.1161/CIRCEP.120.009747
Item in Clipboard
Clinical Trial
Durable Physiological Changes and Decreased Syncope Burden 12 Months After Unifocal Right-Sided Ablation Under Computed Tomographic Guidance in Patients With Neurally Mediated Syncope or Functional Sinus Node Dysfunction
Circ Arrhythm Electrophysiol.
2021 Jun.
Abstract
[Figure: see text].
Trial registration: ClinicalTrials.gov NCT02954666.
Keywords: autonomic nervous system; cohort studies; exercise test; heart rate; syncope.
Figures
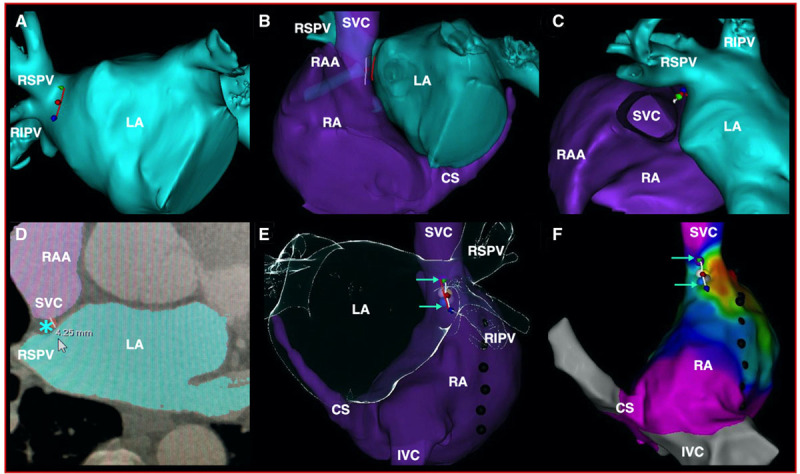
Computed tomography (CT) scan images and electroanatomical map indicating the region targeted during cardioneuromodulation (CardNM). CT scan images (A–E) and electroanatomical map (F) indicating the region targeted during CardNM. A, Red line delineating the mid and caudal parts of the right superior pulmonary vein antrum in an anteroposterior projection. B and C, Target line guiding CardNM indicated by the white line facing the first design line at the superior vena cava (SVC)–right atrium (RA) junction in a modified left anterior oblique (B) and cranial (C) projection. D, Transversal slice at the midportion of the target line showing the location and thickness of the fat pad containing the anterior right ganglionated plexus (ARGP) at this level (blue asterisk). E and F, Ablation tags along the target line in a posteroanterior CT scan view (E) and on the electroanatomical map (F) in the same projection after merging the two images. The region of the ARGP ablated is indicated by 2 green arrows. Each individual ablation is indicated using a colored tag. The phrenic nerve is tagged with black dots. CS indicates coronary sinus; IVC, inferior vena cava; LA, left atrium; RAA, right atrial appendage; RIPV, right inferior pulmonary vein; and RSPV, right superior pulmonary vein.
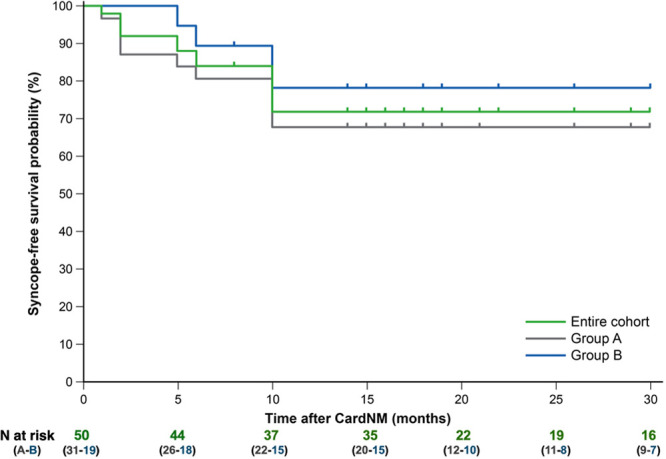
Syncope-free survival curves. CardNM indicates cardioneuromodulation.
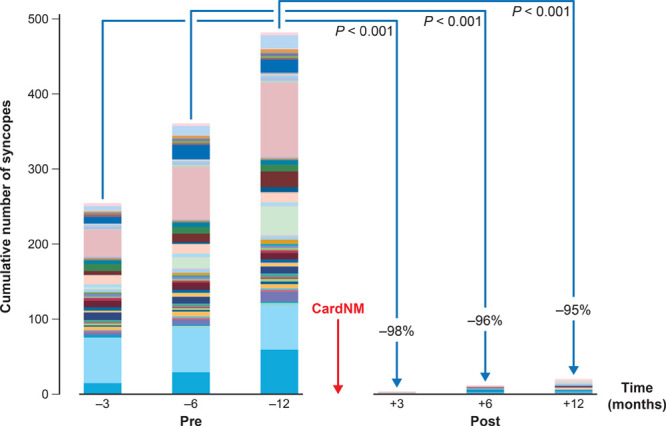
Syncope burden at 3, 6, and 12 mo before and after cardioneuromodulation (CardNM). Each patient is represented by a different color.
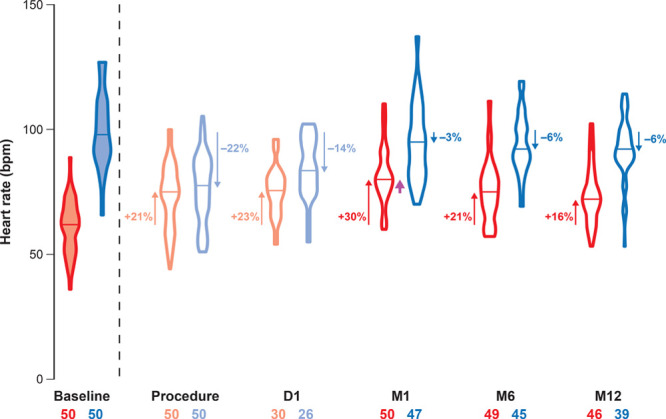
Basal heart rate (HR) and HR after atropine injection. Basal HRs are represented by red violin plots. Reset basal HRs after ablation and 1 d later are represented by pale-red violin plots. Corresponding HRs after atropine are shown by the blue and pale-blue violin plots. The median value is mentioned for each violon plot by a horizontal line. The number of patients involved (X–X) and level of the median HR modification compared with baseline (%) are shown. HR acceleration (upward arrows) or deceleration (downward arrows) were all significant compared with baseline (P<0.001). The median basal HR at M6 and M12 was comparable with the postprocedural basal HR while the median basal HR at M1 was significantly higher (purple arrow; P<0.001). D indicates day; and M, month.
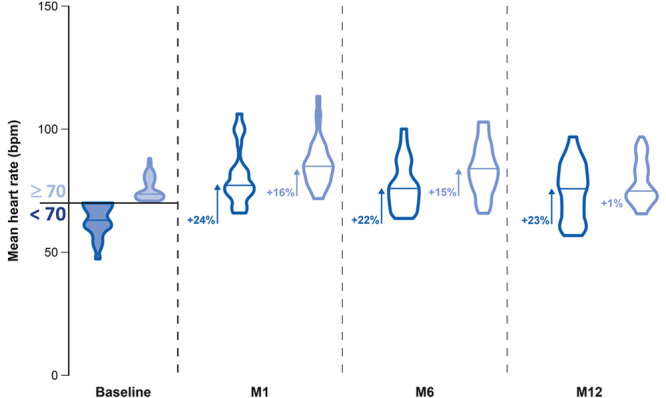
Mean heart rate (HR) during 24-h rhythm registration of patients with a mean HR at baseline under or above 70 beats per minute (bpm) at baseline, M1, M6, and M12. The blue violin plots indicate patients with a mean HR at baseline <70 bpm, and the light blue violin plots indicate these with a mean HR ≥70 bpm. The data are presented at baseline, M1, M6, and M12. The median values are indicated by the horizontal line in each violin plot. The level of HR acceleration compared with baseline is indicated in percentage. Significant values (P<0.001) compared with baseline are indicated by arrows. M indicates month.
References
-
- Shen WK, Sheldon RS, Benditt DG, Cohen MI, Forman DE, Goldberger ZD, Grubb BP, Hamdan MH, Krahn AD, Link MS, et al. . 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2017;136:e25–e59. doi: 10.1161/CIR.0000000000000498 - PubMed
-
- Brignole M, Moya A, de Lange FJ, Deharo JC, Elliott PM, Fanciulli A, Fedorowski A, Furlan R, Kenny RA, Martin A, et al. . 2018 ESC Guidelines for the diagnosis and management of syncope. Eur Heart J. 2018;39:1883–1948. - PubMed
-
- Pachon JC, Pachon EI, Pachon JC, Lobo TJ, Pachon MZ, Vargas RN, Jatene AD. “Cardioneuroablation”–new treatment for neurocardiogenic syncope, functional AV block and sinus dysfunction using catheter RF-ablation. Europace. 2005;7:1–13. doi: 10.1016/j.eupc.2004.10.003 - PubMed
-
- Pachon JC, Pachon EI, Cunha Pachon MZ, Lobo TJ, Pachon JC, Santillana TG. Catheter ablation of severe neurally meditated reflex (neurocardiogenic or vasovagal) syncope: cardioneuroablation long-term results. Europace. 2011;13:1231–1242. doi: 10.1093/europace/eur163 - PubMed
-
- Yao Y, Shi R, Wong T, Zheng L, Chen W, Yang L, Huang W, Bao J, Zhang S. Endocardial autonomic denervation of the left atrium to treat vasovagal syncope: an early experience in humans. Circ Arrhythm Electrophysiol. 2012;5:279–286. doi: 10.1161/CIRCEP.111.966465 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
