

Determinants of maternal near miss among women admitted to maternity wards of tertiary hospitals in Southern Ethiopia, 2020: A hospital-based case-control study
- PMID: 33999941
- PMCID: PMC8128231
- DOI: 10.1371/journal.pone.0251826
Determinants of maternal near miss among women admitted to maternity wards of tertiary hospitals in Southern Ethiopia, 2020: A hospital-based case-control study
Abstract
Background: A maternal near-miss (MNM) refers to when a gravely ill woman survives a complication as a result of the standard of care she receives or by chance during gestation, childbirth, or within 42 days of the termination of pregnancy. Rescuers of near-miss events share several features with mothers who have died and identifying MNM determinants will aid in improving the capacity of the health system to reduce severe maternal morbidity and mortality. Ethiopia is one of the countries in sub-Saharan Africa with high maternal mortality and morbidity, but there is little evidence on determinants of a MNM based on a WHO criteria. Hence, this study aimed at identifying determinants of MNM among women admitted to tertiary hospitals in southern Ethiopia, 2020.
Methods: A facilities-based unmatched case-control study was conducted in five selected tertiary hospitals found in central southern Ethiopia from February 1 to June 1, 2020. A total of 322 (81 cases and 241 controls) study participants were included in the study. At the time of their discharge, cases were recruited consecutively, while controls were selected using a systematic sampling method. The cases were women admitted to hospitals during pregnancy, childbirth, or 42 days following termination of pregnancy who met at least one of the WHO near-miss criteria. Whereas the controls comprised of women who were admitted during pregnancy, childbirth, or 42 days following termination of pregnancy and discharged without severe obstetric complications. Data collection was conducted using the interviewer-administered structured questionnaire and data abstraction tool. The data was coded and entered into Epi-Data version 3.1 and exported to SPSS version 23 for analysis. Multivariable logistic regression analysis was conducted and determinants of MNM were established at p-value<0.05.
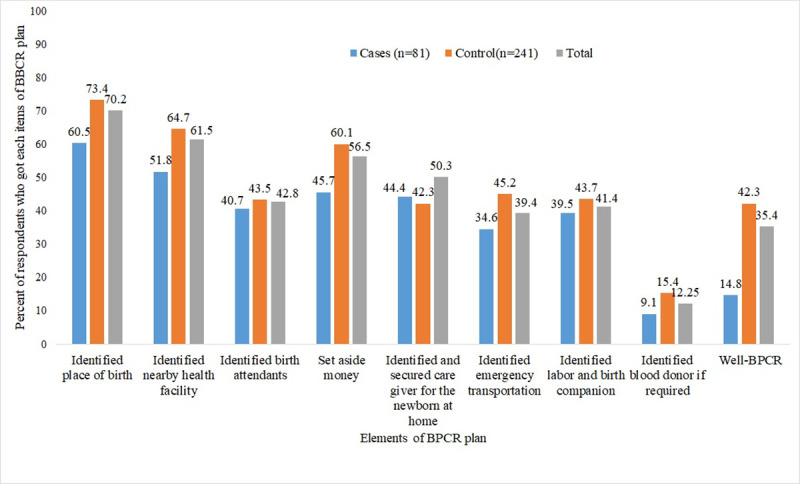
Results: Severe postpartum hemorrhage (50.6%) and sepsis (23.4%) were the most common reasons for admission of cases. Lack of ANC [AOR = 3.25; 95%CI: 2.21,7.69], prior history of Cesarean section [AOR = 3.53; 95%CI:1.79,6.98], delaying more than 60 minute to access final place of care [AOR = 3.21; 95%CI:1.61,6.39], poor practice of Birth preparedness and complication readiness (BPCR) [AOR = 3.31; 95%CI:1.50,7.29], and history of preexisting medical disorders [AOR = 2.79; 95%CI:1.45,5.37] were identified as significantly determinants of maternal near miss.
Conclusion and recommendation: Stakeholders need to enhance their efforts for improving access to roads and transportations. Besides, women who have a prior history of Caesarean section, chronic medical conditions, and no ANC need special attention from their families and health care providers to proactively mitigate the occurrence of serious obstetric complications. More attention has to be paid to birth preparedness and complication readiness activities.
Conflict of interest statement
The authors have declared that no competing interests exist
Figures
References
-
- WHO, U., UNFPA, World Bank Group, and the United Nations Population Division. Trends in Maternal Mortality: 2000 to 2017. Geneva. World Health Organization, 2019.
-
- Alkema L., et al., United Nations Maternal Mortality Estimation Inter-Agency Group collaborators and technical advisory group. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet, 2016. 387(10017): p. 462–474. 10.1016/S0140-6736(15)00838-7 - DOI - PMC - PubMed
-
- WHO, U., UNFPA, World Bank Group and the United Nations Population Division; Internationally comparable MMR estimates by the Maternal Mortality Estimation Inter-Agency Group (MMEIG); Maternal mortality in 2000–2017: Ethiopia.
-
- The World Health Organization (WHO). Evaluating the quality of care for severe pregnancy complications. The WHO near-miss approach for maternal health. Geneva: World Health Organization; 2011.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
