

Chronic fusiform extracranial vertebral artery aneurysm with recurrent posterior circulation emboli: Case report and review of the literature
- PMID: 34000865
- PMCID: PMC8902263
- DOI: 10.1177/15910199211018581
Chronic fusiform extracranial vertebral artery aneurysm with recurrent posterior circulation emboli: Case report and review of the literature
Abstract
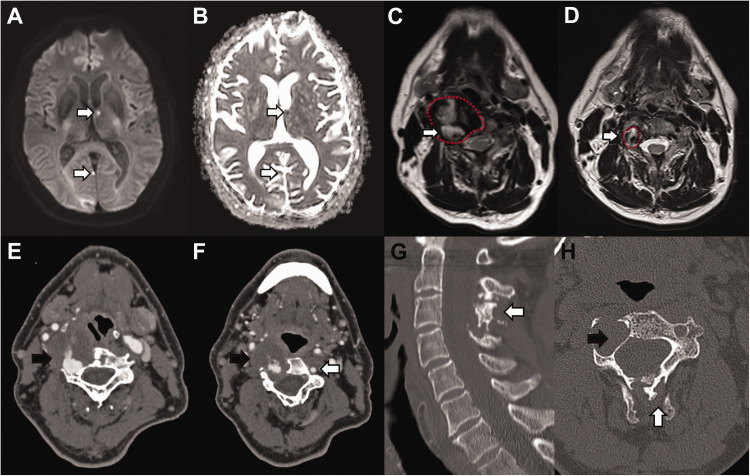
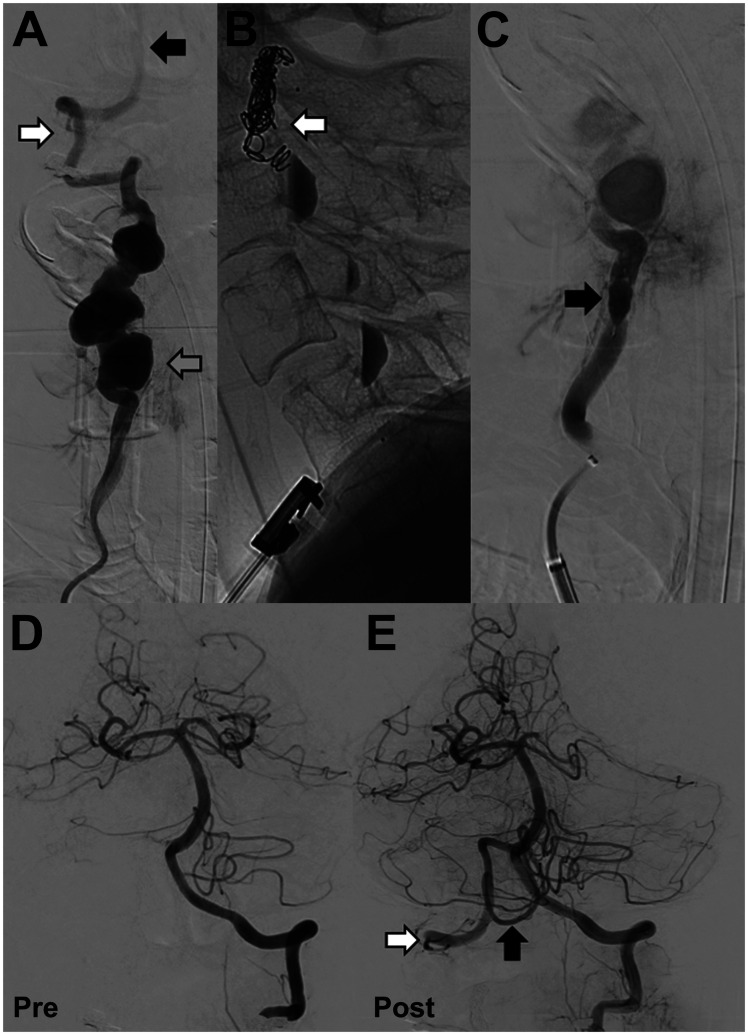
We report a case of a 64-year-old man with a fusiform right extracranial vertebral artery aneurysm, spanning over half the extra-cranial V2 (foraminal) segment, presenting with recurrent multi-focal posterior circulation embolic ischaemic stroke. The patient was treated with endovascular embolisation of the right vertebral artery to prevent further thrombo-embolic events. Distal and proximal occlusion of the aneurysmal vertebral artery was performed with a micro-vascular plug with partial aneurysm sack embolisation to aid thrombosis and reduce the risk of recanalisation. Two months post procedure MR angiography confirmed successful aneurysm occlusion with no post-procedural complication. The patient returned to his normal independent life. Endovascular treatment with vessel sacrifice is an effective treatment with low morbidity and we believe the MVP device to be a efficacious option in the vertebral artery.
Keywords: Vertebral artery; aneurysm; dissection; embolisation; embolism; stroke.
Conflict of interest statement
Figures
References
-
- Krueger BR, Okazaki H. Vertebral-basilar distribution infarction following chiropractic cervical manipulation. Mayo Clin Proc 1980; 55: 322–332. - PubMed
-
- Do KH, Leggit JC, Galifianakis A. Extracranial vertebral artery dissecting aneurysm with snowboarding: a case report. Curr Sports Med Rep 2018; 17: 16–19. - PubMed
-
- Egnor MR, Page LK, David C. Vertebral artery aneurysm – a unique hazard of head B banging by heavy metal rockers. Pediatr Neurosurg 1991; 17: 135–138. - PubMed
-
- Schievink WI, Piepgras DG. Cervical vertebral artery aneurysms and arteriovenous fistulae in neurofibromatosis type 1: case reports. Neurosurgery 1991; 29: 760–765. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
