

Italian onco-haematological patients' preferences in bad news communication: a preliminary investigation
- PMID: 34001021
- PMCID: PMC8127256
- DOI: 10.1186/s12885-021-08181-0
Italian onco-haematological patients' preferences in bad news communication: a preliminary investigation
Abstract
Background: The manner in which bad news is communicated in oncological contexts can affect patients' engagement, their coping strategies and therapeutic compliance. Although this topic has been broadly investigated since the nineties, to the best of our knowledge, little has been written about Italian patients' experiences and preferences concerning what the oncologists should disclose and how they should intimate patients about their health conditions in different stages of oncological disease.
Methods: In an attempt to fill this gap, an online self-report questionnaire was administered to a sample of Italian onco-haematological patients. Data were analysed both qualitatively (by a content analysis) and quantitatively (by descriptive analysis and Generalized Linear Mixed Model).
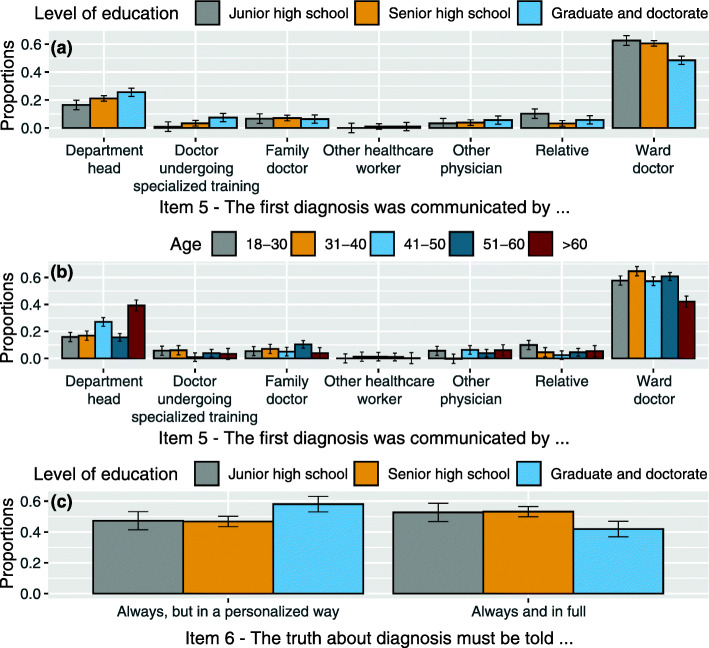
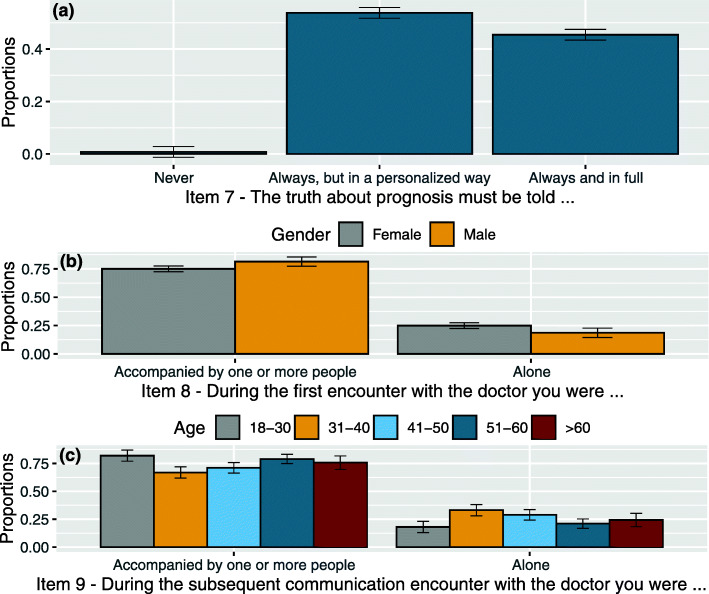
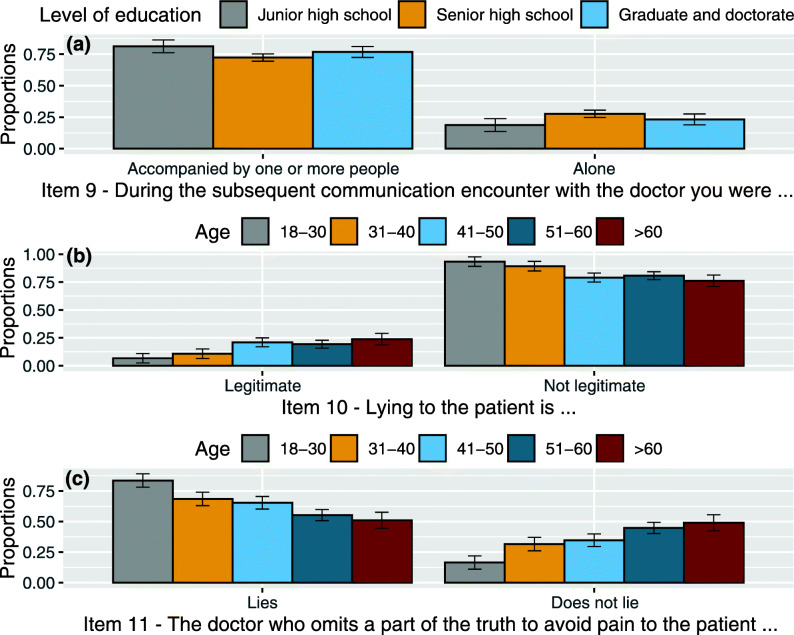
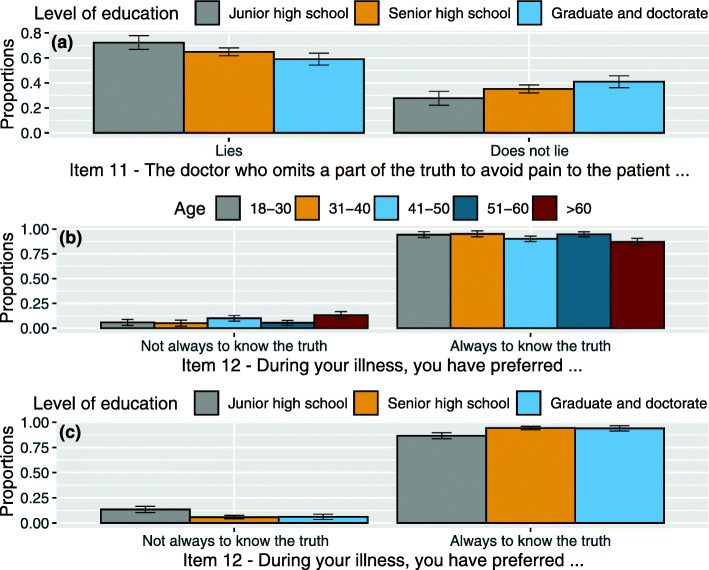
Results: While the majority of patients elected to know the truth during their clinical course, a polarisation between those arguing that the truth be fully disclosed and those claiming that the truth be communicated in a personalised way was observed at the attitude level. Among demographic variables accounted for, age seems to most affect patients' preferences. Indeed, younger Italian patients decidedly reject concealment of the truth, even when justified by the beneficence principle. This result could be a reaction to some protective and paternalistic behaviours, but it could even reflect a relation according to which the more the age increases the more the fear of knowing rises, or an intergenerational change due to different ways of accessing the information. The qualitative analysis of the final open-ended question revealed three main sources of problems in doctor-patient encounters: scarcity of time, absence of empathy and use of not-understandable language that makes it difficult for patients to assume a more active role.
Conclusions: The results of the present study, which represents a preliminary step in the subject investigation, will be deployed for the construction and validation of a more sophisticated questionnaire. Better awareness of the Italian onco-haematological patients' preferences concerning bad news communication and truth-telling could be useful in adopting more suitable medical practices and improving doctor-patient relationships.
Keywords: Bad news; Onco-haematological disease; Patients’ experiences; Patients’ preferences; Truth.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Assessing patients´ preferences for breaking Bad News according to the SPIKES-Protocol: the MABBAN scale.Patient Educ Couns. 2020 Aug;103(8):1623-1629. doi: 10.1016/j.pec.2020.02.036. Epub 2020 Feb 27. Patient Educ Couns. 2020. PMID: 32151521
-
Experiences of truth disclosure in terminally ill cancer patients in palliative home care.Palliat Support Care. 2011 Jun;9(2):173-80. doi: 10.1017/S1478951511000046. Palliat Support Care. 2011. PMID: 24468485
-
Cancer patients' experiences and preferences when receiving bad news: a qualitative study.J Cancer Res Clin Oncol. 2023 Jul;149(7):3859-3870. doi: 10.1007/s00432-022-04311-8. Epub 2022 Aug 23. J Cancer Res Clin Oncol. 2023. PMID: 35999331 Free PMC article.
-
[Are schizophrenic patients being told their diagnosis today in France?].Encephale. 2017 Apr;43(2):160-169. doi: 10.1016/j.encep.2016.01.011. Epub 2016 Jun 29. Encephale. 2017. PMID: 27372353 Review. French.
-
[Communication preferences of patients with prostate cancer : Preferences regarding the communication of bad news of patients with prostate cancer in Germany-results of an anonymous patient survey].Urologe A. 2016 Oct;55(10):1339-1346. doi: 10.1007/s00120-016-0154-x. Urologe A. 2016. PMID: 27306355 Review. German.
Cited by
-
Validation of the EORTC information (QLQ-INFO25) and satisfaction with care (IN-PATSAT32) modules in the Polish cancer patient population.BMC Health Serv Res. 2025 Feb 13;25(1):241. doi: 10.1186/s12913-025-12382-9. BMC Health Serv Res. 2025. PMID: 39939847 Free PMC article.
References
-
- Donovan K. Breaking Bad News. In: Communication Bad News. Behavioral Science Learning Modules. Division of Mental Health: World Health Organization; 1993. p. 1–14.
-
- Fields SA, Johnson MW. Physician-patient communication: breaking bad news. W V Med J. 2012;108(2):32–36. - PubMed
-
- Borjalilu S, Karbakhsh M, Mirsharifi R, Davoodzadeh K, Aghili M, Kaviani A. Measuring Attitude and Practice of Physician toward Breaking Bad News to the Breast Cancer Patients: Development and Validation of a Questionnaire. Arch Breast Cancer. 2016;3(2):41–49. doi: 10.19187/abc.20163241-49. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
