

Ambient bright light treatment improved proxy-rated sleep but not sleep measured by actigraphy in nursing home patients with dementia: a placebo-controlled randomised trial
- PMID: 34001024
- PMCID: PMC8127192
- DOI: 10.1186/s12877-021-02236-4
Ambient bright light treatment improved proxy-rated sleep but not sleep measured by actigraphy in nursing home patients with dementia: a placebo-controlled randomised trial
Abstract
Background: Up to 70% of nursing home patients with dementia suffer from sleep problems. Light is the main zeitgeber to the circadian system and thus has a fundamental impact on sleep-wake behaviour. Low indoor light levels in nursing homes have been reported, and in combination with age-related reductions in light sensitivity, insufficient light exposure is likely to contribute to sleep problems in this population. Increasing daytime light exposure using bright light treatment (BLT) may represent a feasible non-pharmacological treatment for sleep problems in nursing home patients with dementia.
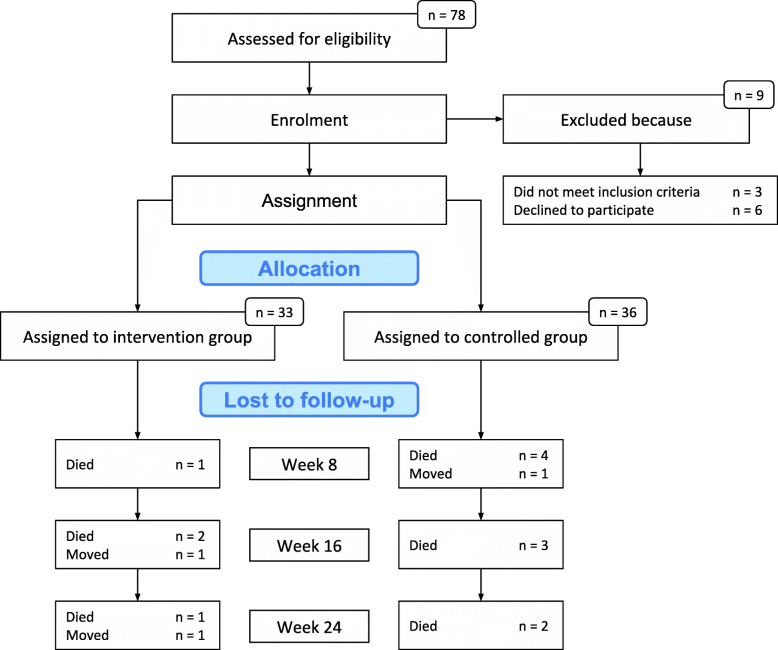
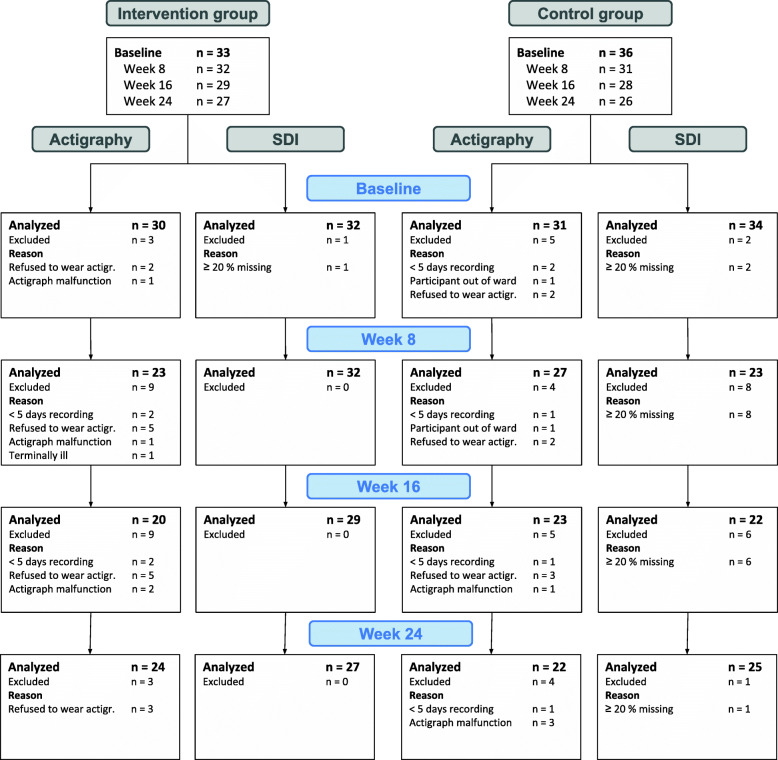
Methods: The present study reports on sleep outcomes, which are the primary outcomes of the DEM.LIGHT trial (Therapy Light Rooms for Nursing Home Patients with Dementia- Designing Diurnal Conditions for Improved Sleep, Mood and Behavioural Problems), a 24-week cluster-randomised placebo-controlled trial including 8 nursing home units and 69 resident patients. The intervention comprised ambient light of 1000 lx and 6000 K from 10:00 to 15:00, with gradually increasing and decreasing light levels prior to and following this interval, using ceiling mounted light-fixtures and light emitting diode technology. The placebo condition had continuous standard light levels (150-300 lx, ~ 3000 K). Sleep was assessed at baseline and follow-up at week 8, 16, and 24, using the proxy-rated Sleep Disorder Inventory (SDI) and actigraphy (Actiwatch II, Philips Respironics). Mixed linear models were used to evaluate intervention effects, adjusting for relevant covariates such as age, gender, number of drugs, severity of dementia, eye disease, and estimated light exposure.
Results: Sleep as measured by the SDI was significantly improved in the intervention group compared to the control group from baseline to week 16 (B = - 0.06, 95% CI -0.11 - -0.01, p < .05) and from baseline to week 24 (B = - 0.05, 95% CI -0.10 - -0.01, p < .05). There was no effect according to the SDI at week 8 and no significant effects in terms of actigraphically measured sleep.
Conclusions: Proxy-rated sleep improved among nursing home patients with dementia following 16 and 24 weeks of BLT. These improvements were not corroborated by actigraphy recordings.
Trial registration: ClinicalTrials.gov Identifier: NCT03357328 . Registered 29 November 2017 - Retrospectively registered.
Keywords: Actigraphy; Dementia; Nursing home; Sleep; Sleep disorder inventory.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- American Psychiatric Association. Neurocognitive disorders. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington DC; 2013.
-
- World Health Organization. Dementia [Internet]. 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/dementia
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
