

Awareness screening and referral patterns among pediatricians in the United States related to early clinical features of spinal muscular atrophy (SMA)
- PMID: 34001052
- PMCID: PMC8127310
- DOI: 10.1186/s12887-021-02692-2
Awareness screening and referral patterns among pediatricians in the United States related to early clinical features of spinal muscular atrophy (SMA)
Abstract
Background: Spinal Muscular Atrophy (SMA), a leading genetic cause of death in infants, is an autosomal recessive neuromuscular disease characterized by progressive muscle weakness and atrophy. While early diagnosis of SMA is critical to modifying disease progression and improving outcomes, serious diagnostic delays persist. There is a need to improve SMA awareness, screening, and referral patterns.
Methods: Two online surveys, developed by Cure SMA for general pediatricians, were distributed by Medscape Education via email (September 2018, n = 300, December 2019, n = 600). The surveys asked about adherence to the American Academy of Pediatrics (AAP) developmental screening and surveillance guidelines, comfort with identification of early signs of neuromuscular disease (NMD), familiarity with SMA, and barriers to timely referral.
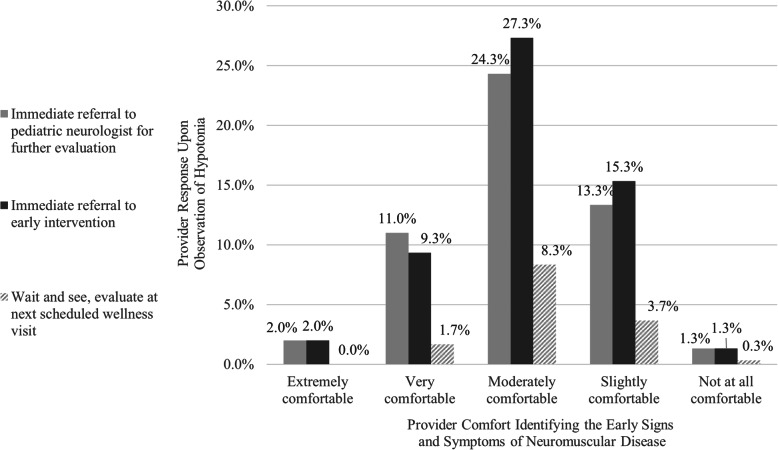
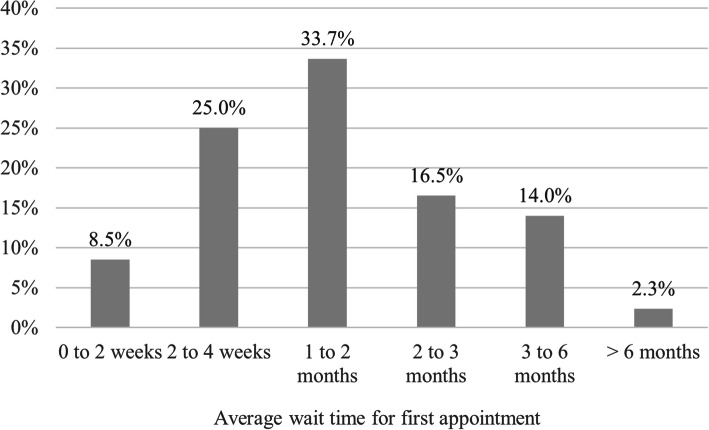
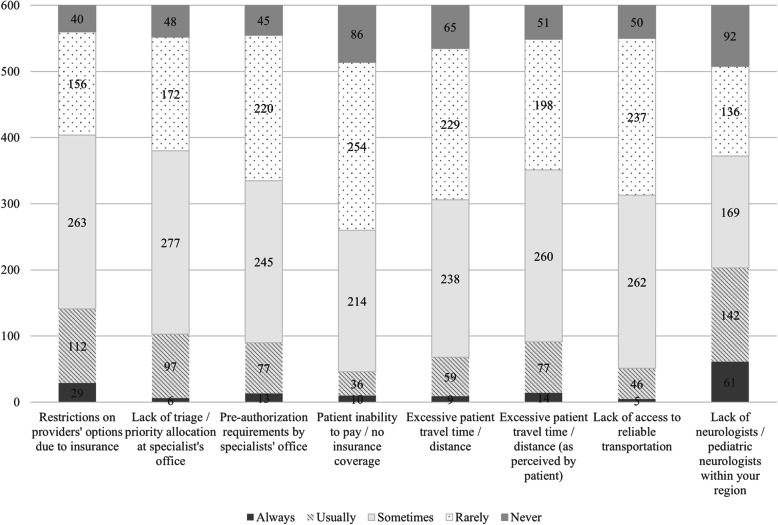
Results: In 2018, 70.3% of survey respondents indicated comfort in identifying early signs of NMD and 67.3% noted familiarity with SMA. 52.7% correctly indicated the need for genetic testing to make a definitive diagnosis of SMA, 74.0% meet or exceed developmental screening recommendations, and 52.0% said they would immediately refer to a specialist. In 2019, with a larger sample, 73.0% adhere to developmental screening guidelines, and awareness of the genetic testing requirement for SMA was significantly lower by 7.7% (p < 0.03). Specialist wait times emerged as a barrier to referral, with 64.2% of respondents citing wait times of 1-6 months.
Conclusions: Many pediatricians underutilize developmental screening tools and lack familiarity with diagnostic requirements for SMA. Continuing efforts to expand awareness and remove barriers to timely referral to SMA specialists, including reducing appointment wait times, are needed.
Conflict of interest statement
The authors have no competing interests to disclose.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
