

Clinical characteristics and surgical treatment of ureteral endometriosis: our experience with 40 cases
- PMID: 34001081
- PMCID: PMC8130255
- DOI: 10.1186/s12905-021-01349-7
Clinical characteristics and surgical treatment of ureteral endometriosis: our experience with 40 cases
Abstract
Background: To present the experience with the surgical management of ureteral endometriosis (UE) in our single center.
Methods: To present the experience with the surgical management of ureteral endometriosis (UE) in our single center. A retrospective analysis of 40 patients with UE who presented with intraoperative surgical findings of endometriosis involving the ureter and pathology-proven UE was performed.
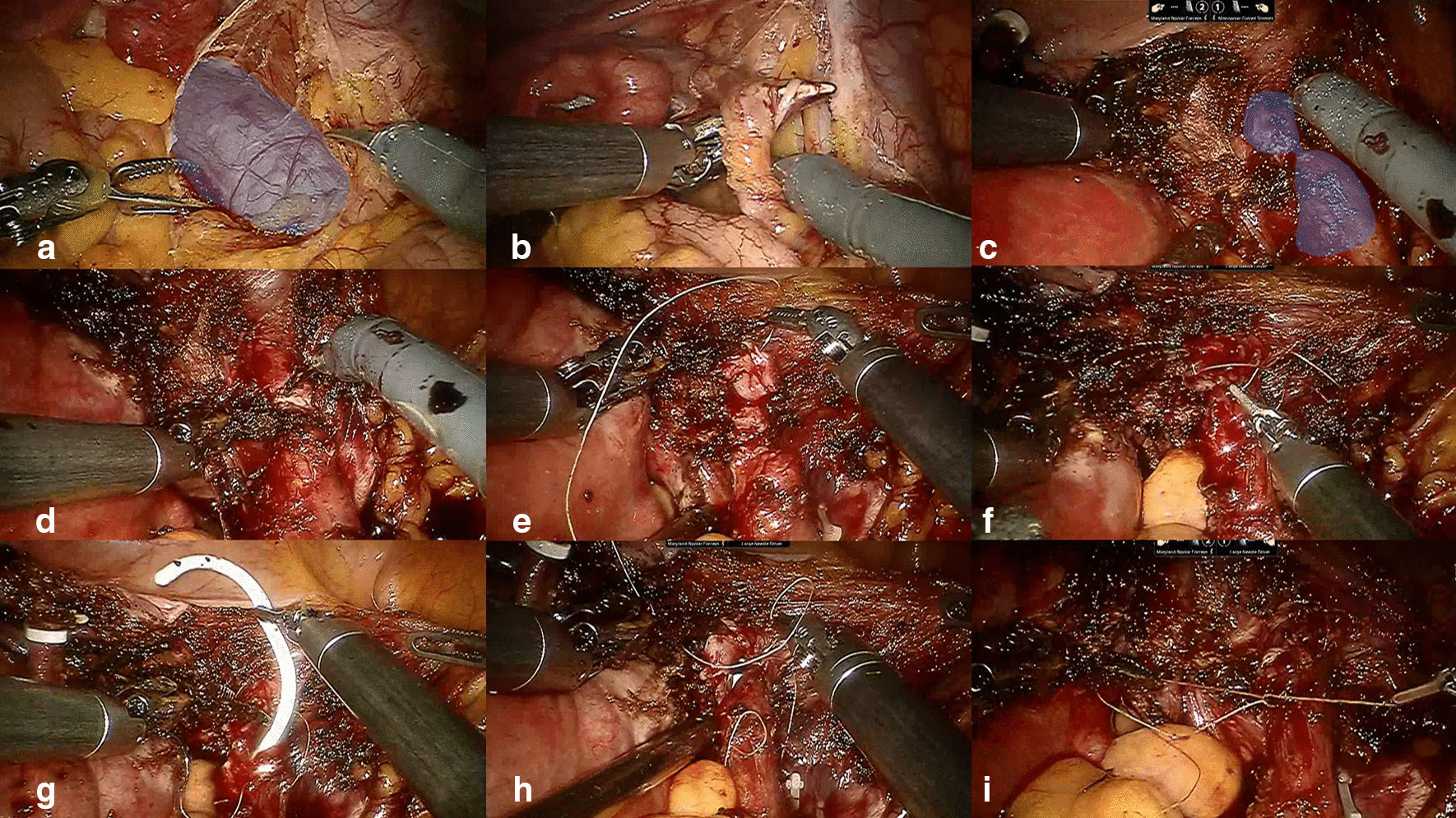
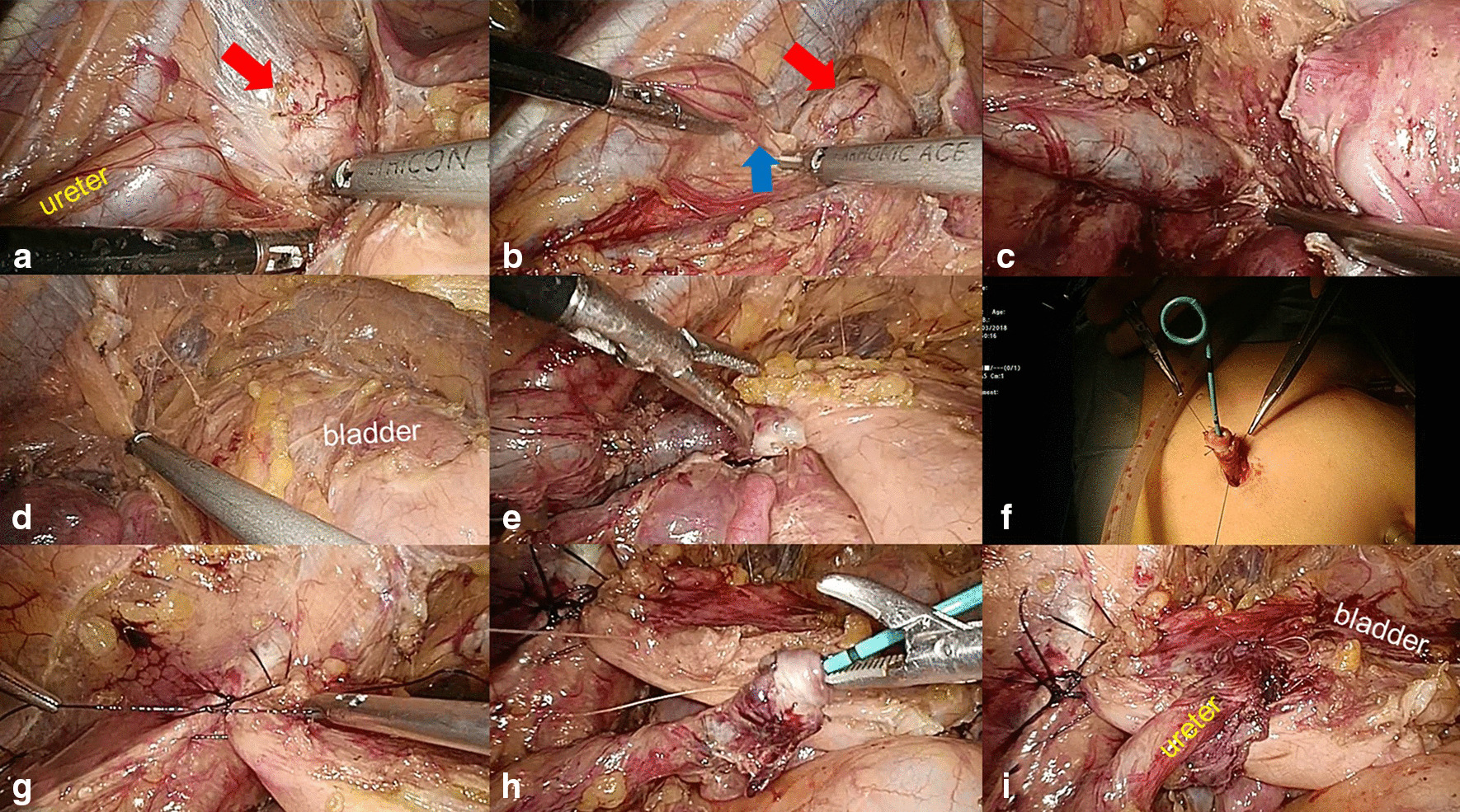
Results: Forty patients (median age, 42.5 years) with histological evidence of UE were included. Six (15%) patients had a history of endometriosis. Twenty-one (52%) patients had urological symptoms, and 19 (48%) patients were asymptomatic. All patients had hydronephrosis. The mean glomerular filtration rate (GFR) of the ipsilateral kidney was significantly worse than that of the contralateral kidney (23.4 vs 54.9 ml/min; P < 0.001). Twelve (30%) patients were treated with ureteroureterostomy (11 open approaches and 1 robotic approach). Twenty-two (55%) patients underwent ureteroneocystostomy (17 open approaches, 4 laparoscopic approaches and 1 robotic approach). Five patients underwent nephroureterectomy. One patient refused aggressive surgery and received ureteroscopic biopsy and ureteral stent placement. Thirteen (33%) patients required gynecological operations. Three (8%) patients in the open group suffered from major surgical complications. Nine (24%) patients received postoperative endocrine therapy. Twenty-eight (70%) patients were followed up (median follow-up time, 71 months). Twenty-four patients received kidney-sparing surgeries. The success rate for these 24 patients was 21/24 (87.5%). The success rates of ureteroneocystostomy and ureteroureterostomy were 15/16 (93.8%) and 5/7 (71.4%), respectively.
Conclusions: Although UE is rare, we should remain vigilant for the disease among female patients with silent hydronephrosis. Typically, a multidisciplinary surgical team is necessary. For patients with severe UE, segmental ureteral resection with ureteroureterostomy (UU) or ureteroneocystostomy may be a preferred choice.
Keywords: Case report; Nephroureterectomy; Ureteralendometriosis; Ureteroneocystostomy; Ureteroureterostomy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
