

Evaluation of a serum-based antigen test for tuberculosis in HIV-exposed infants: a diagnostic accuracy study
- PMID: 34001096
- PMCID: PMC8130139
- DOI: 10.1186/s12916-021-01983-w
Evaluation of a serum-based antigen test for tuberculosis in HIV-exposed infants: a diagnostic accuracy study
Abstract
Background: Non-sputum methods are urgently needed to improve tuberculosis diagnosis and treatment monitoring in children. This study evaluated the ability of a serum assay quantifying a species-specific peptide of the Mycobacterium tuberculosis CFP-10 virulence factor via nanotechnology and matrix-assisted laser desorption ionization time-of-flight mass spectrometry to diagnose tuberculosis in HIV-infected and HIV-uninfected infants.
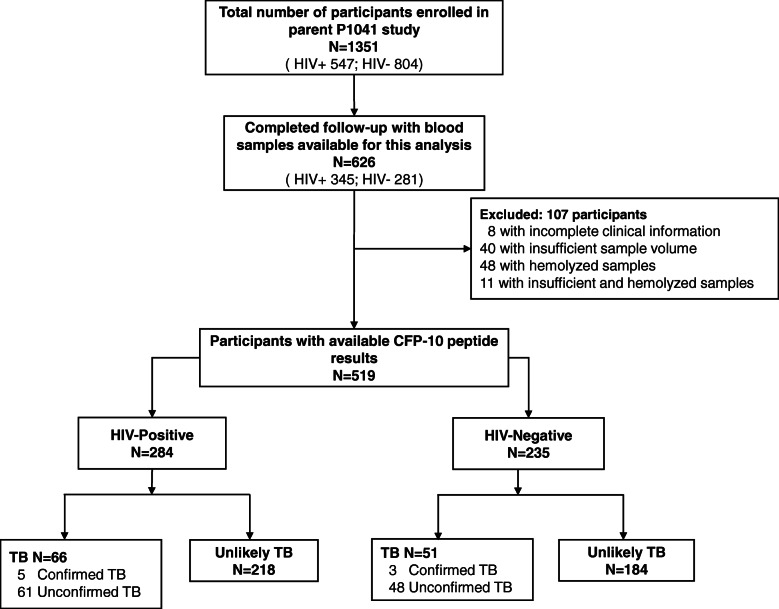
Methods: Serum CFP-10 peptide signal was blinded evaluated in cryopreserved sera of 519 BCG-immunized, HIV-exposed infants (284 HIV-infected, 235 HIV-uninfected) from a multi-center randomized placebo-controlled isoniazid prophylaxis trial conducted in southern Africa between 2004 and 2008, who were followed up to 192 weeks for Mtb infection and TB. Children were classified as confirmed, unconfirmed, or unlikely tuberculosis cases using 2015 NIH diagnostic criteria for pediatric TB.
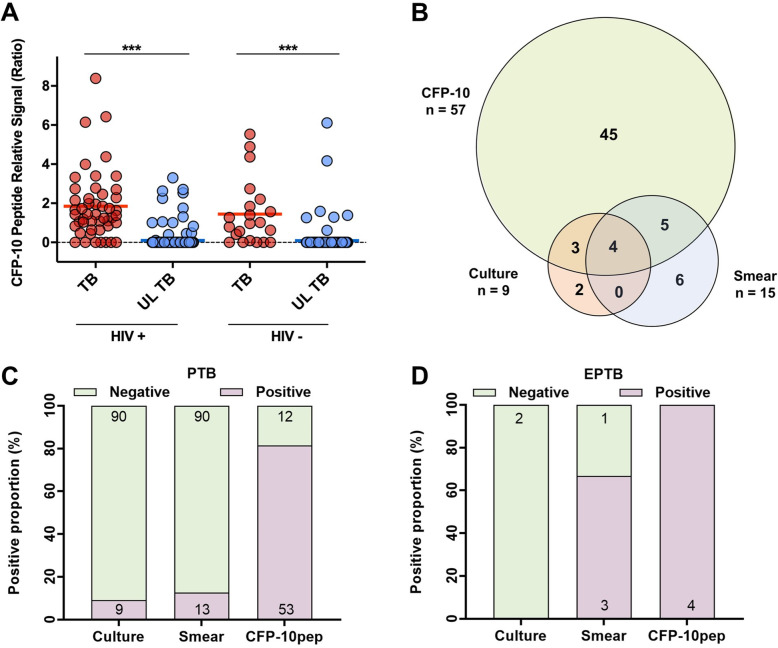
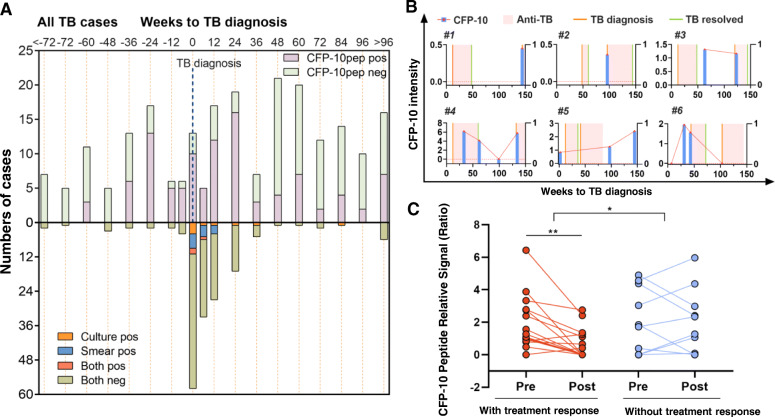
Results: In HIV-infected infants, CFP-10 signal had 100% sensitivity for confirmed TB (5/5, 95% CI, 47.8-100) and 83.7% sensitivity for unconfirmed TB (36/43, 95% CI 69.3-93.2), with 93.1% specificity (203/218, 95% CI 88.9-96.1). In HIV-uninfected infants, CFP-10 signal detected the single confirmed TB case and 75.0% of unconfirmed TB cases (15/20; 95% CI 50.9-91.3), with 96.2% specificity (177/184, 95% CI, 92.3-98.5). Serum CFP-10 achieved 77% diagnostic sensitivity for confirmed and unconfirmed TB (13/17, 95% CI, 50-93%) at ≤ 24 weeks pre-diagnosis, and both CFP-10-positivity and concentration declined following anti-TB therapy initiation.
Conclusions: Serum CFP-10 signal exhibited high diagnostic sensitivity and specificity for tuberculosis in HIV-infected and HIV-uninfected infants and potential utility for early TB detection and monitoring of anti-TB treatment responses.
Keywords: CFP-10; Mass spectrometry; Nanotechnology; Pediatric tuberculosis.
Conflict of interest statement
Y. H, C.L. and C.J.L. report other support from NanoPin Technologies, Inc., outside the submitted work; In addition, Y. H. has a patent “Compositions and methods of determining a level of active
Figures
Similar articles
-
Rapid diagnosis of new and relapse tuberculosis by quantification of a circulating antigen in HIV-infected adults in the Greater Houston metropolitan area.BMC Med. 2017 Nov 1;15(1):188. doi: 10.1186/s12916-017-0952-z. BMC Med. 2017. PMID: 29089034 Free PMC article.
-
Infant TB Infection Prevention Study (iTIPS): a randomised trial protocol evaluating isoniazid to prevent M. tuberculosis infection in HIV-exposed uninfected children.BMJ Open. 2020 Jan 21;10(1):e034308. doi: 10.1136/bmjopen-2019-034308. BMJ Open. 2020. PMID: 31969368 Free PMC article. Clinical Trial.
-
[Evolution of IGRA researches].Kekkaku. 2008 Sep;83(9):641-52. Kekkaku. 2008. PMID: 18979999 Review. Japanese.
-
A CD4+ TNF+ monofunctional memory T-cell response to BCG vaccination is associated with Mycobacterium tuberculosis infection in infants exposed to HIV.EBioMedicine. 2022 Jun;80:104023. doi: 10.1016/j.ebiom.2022.104023. Epub 2022 May 6. EBioMedicine. 2022. PMID: 35533496 Free PMC article. Clinical Trial.
-
[Characteristics of a diagnostic method for tuberculosis infection based on whole blood interferon-gamma assay].Kekkaku. 2006 Nov;81(11):681-6. Kekkaku. 2006. PMID: 17154047 Review. Japanese.
Cited by
-
Review and Updates on the Diagnosis of Tuberculosis.J Clin Med. 2022 Sep 30;11(19):5826. doi: 10.3390/jcm11195826. J Clin Med. 2022. PMID: 36233689 Free PMC article. Review.
-
Exploring the Potential of Nanotechnology in Pediatric Healthcare: Advances, Challenges, and Future Directions.Pharmaceutics. 2023 May 24;15(6):1583. doi: 10.3390/pharmaceutics15061583. Pharmaceutics. 2023. PMID: 37376032 Free PMC article. Review.
-
Antibodies as key mediators of protection against Mycobacterium tuberculosis.Front Immunol. 2024 Sep 2;15:1430955. doi: 10.3389/fimmu.2024.1430955. eCollection 2024. Front Immunol. 2024. PMID: 39286260 Free PMC article. Review.
-
Antibodies as clinical tools for tuberculosis.Front Immunol. 2023 Dec 14;14:1278947. doi: 10.3389/fimmu.2023.1278947. eCollection 2023. Front Immunol. 2023. PMID: 38162666 Free PMC article. Review.
-
Quantitation of Circulating Mycobacterium tuberculosis Antigens by Nanopore Biosensing in Children Evaluated for Pulmonary Tuberculosis in South Africa.ACS Nano. 2023 Nov 14;17(21):21093-21104. doi: 10.1021/acsnano.3c04420. Epub 2023 Aug 29. ACS Nano. 2023. PMID: 37643288 Free PMC article.
References
-
- World Health Organization . Global tuberculosis report. 2019.
-
- Edwards DJ, Kitetele F, Van Rie A. Agreement between clinical scoring systems used for the diagnosis of pediatric tuberculosis in the HIV era. Int J Tuberc Lung Dis. 2007;11:263–269. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
