

Dead space estimates may not be independently associated with 28-day mortality in COVID-19 ARDS
- PMID: 34001222
- PMCID: PMC8127435
- DOI: 10.1186/s13054-021-03570-0
Dead space estimates may not be independently associated with 28-day mortality in COVID-19 ARDS
Abstract
Background: Estimates for dead space ventilation have been shown to be independently associated with an increased risk of mortality in the acute respiratory distress syndrome and small case series of COVID-19-related ARDS.
Methods: Secondary analysis from the PRoVENT-COVID study. The PRoVENT-COVID is a national, multicenter, retrospective observational study done at 22 intensive care units in the Netherlands. Consecutive patients aged at least 18 years were eligible for participation if they had received invasive ventilation for COVID-19 at a participating ICU during the first month of the national outbreak in the Netherlands. The aim was to quantify the dynamics and determine the prognostic value of surrogate markers of wasted ventilation in patients with COVID-19-related ARDS.
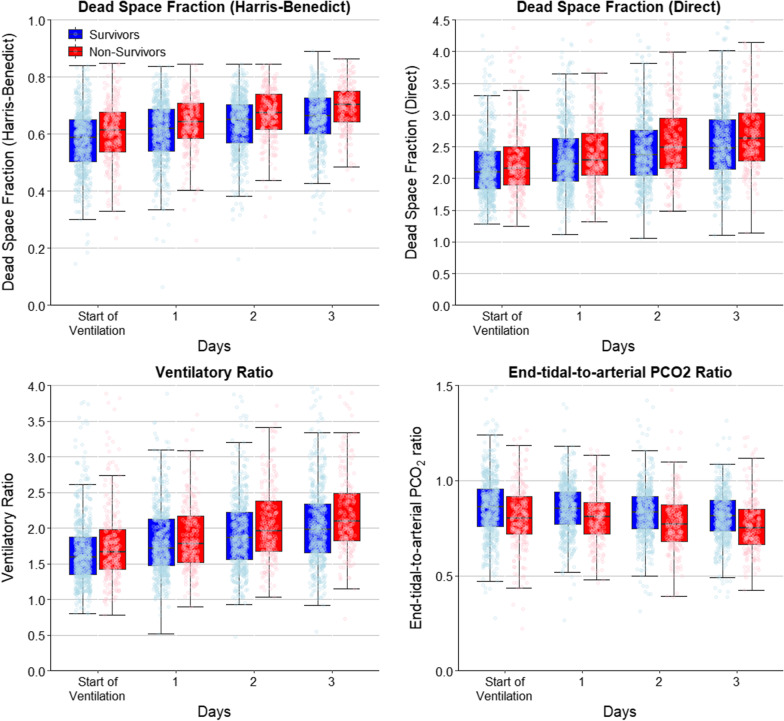
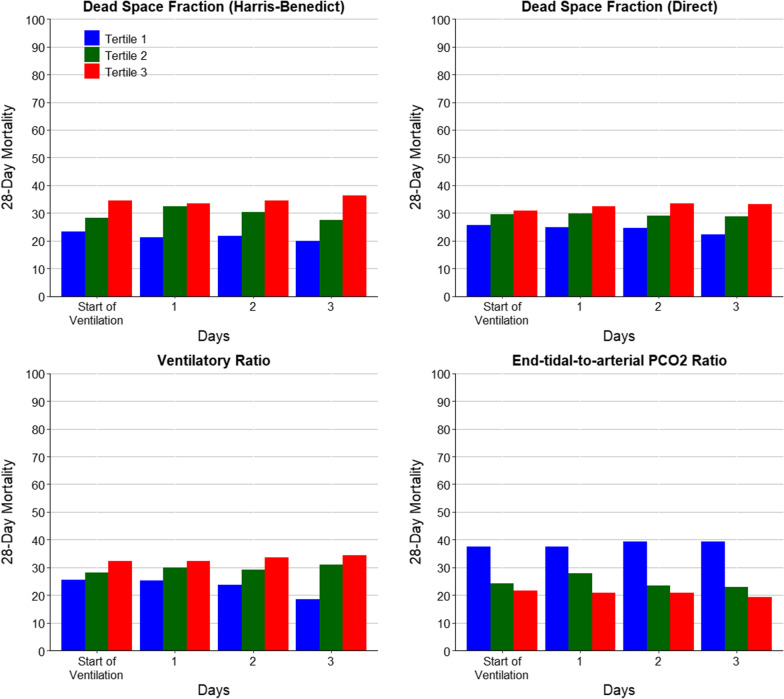
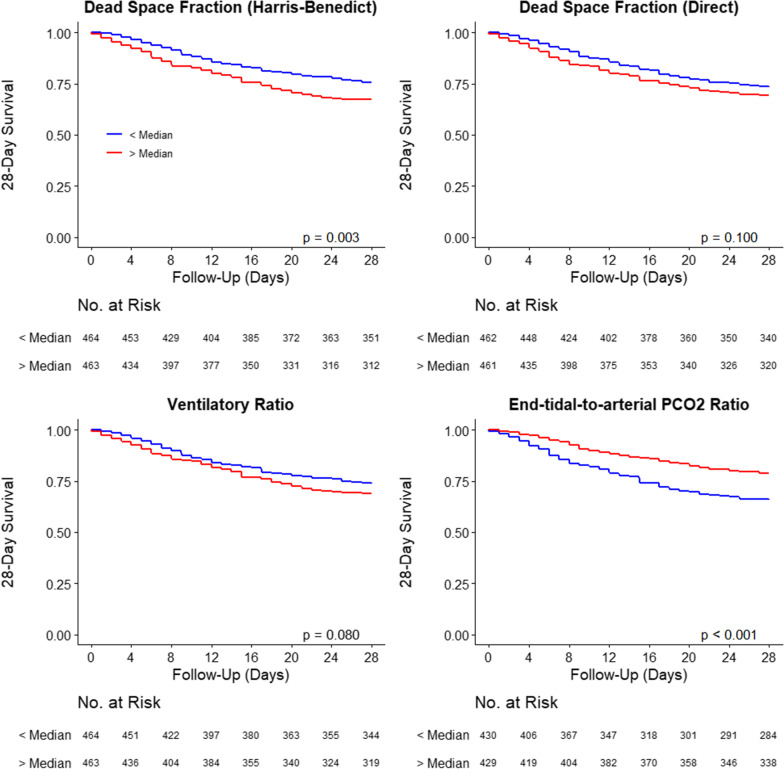
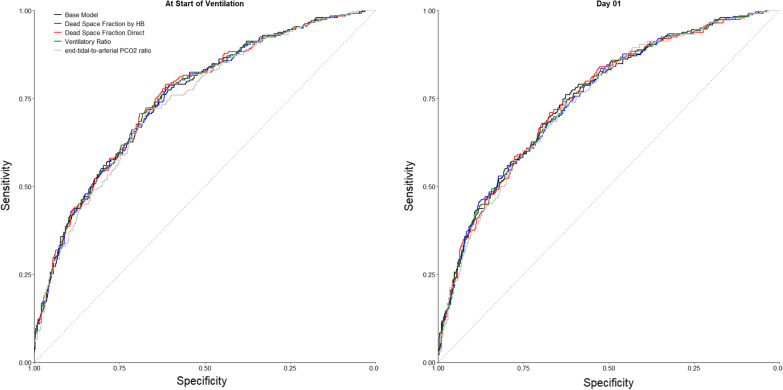
Results: A total of 927 consecutive patients admitted with COVID-19-related ARDS were included in this study. Estimations of wasted ventilation such as the estimated dead space fraction (by Harris-Benedict and direct method) and ventilatory ratio were significantly higher in non-survivors than survivors at baseline and during the following days of mechanical ventilation (p < 0.001). The end-tidal-to-arterial PCO2 ratio was lower in non-survivors than in survivors (p < 0.001). As ARDS severity increased, mortality increased with successive tertiles of dead space fraction by Harris-Benedict and by direct estimation, and with an increase in the VR. The same trend was observed with decreased levels in the tertiles for the end-tidal-to-arterial PCO2 ratio. After adjustment for a base risk model that included chronic comorbidities and ventilation- and oxygenation-parameters, none of the dead space estimates measured at the start of ventilation or the following days were significantly associated with 28-day mortality.
Conclusions: There is significant impairment of ventilation in the early course of COVID-19-related ARDS but quantification of this impairment does not add prognostic information when added to a baseline risk model.
Trial registration: ISRCTN04346342. Registered 15 April 2020. Retrospectively registered.
Keywords: ARDS; Acute respiratory distress syndrome; COVID-19; Dead space; Mortality; Prognostication; Respiratory dead space; Ventilatory ratio.
Conflict of interest statement
Dr Bos receives funding from the Dutch lung foundation (longfonds), from the Innovative Medicine Initiative and from Amsterdam UMC via the AUMC fellowship. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
