

Term Birth Weight and Neurodevelopmental Outcomes
- PMID: 34001752
- PMCID: PMC8439103
- DOI: 10.1097/EDE.0000000000001350
Term Birth Weight and Neurodevelopmental Outcomes
Abstract
Background: Preterm birth is an important risk factor for neurodevelopmental disabilities. The vast majority of these disabilities occur, however, among term births. The role of fetal growth restriction specifically among term babies has been incompletely described.
Methods: We conducted a population-based study of term birth weight and its link to a range of neurodevelopmental outcomes using Norwegian health registries. To remove the influence of preterm birth, we restricted our analyses to 1.8 million singleton babies born during a narrow range of term gestational age (39-41 weeks). Babies with malformations were excluded. We adjusted analyses simply for year of birth, as further adjustments for sex, parity, maternal age, smoking, marital status, immigrant status, and parental education had trivial influence. An additional sibling analysis controlled for unmeasured family-based confounding.
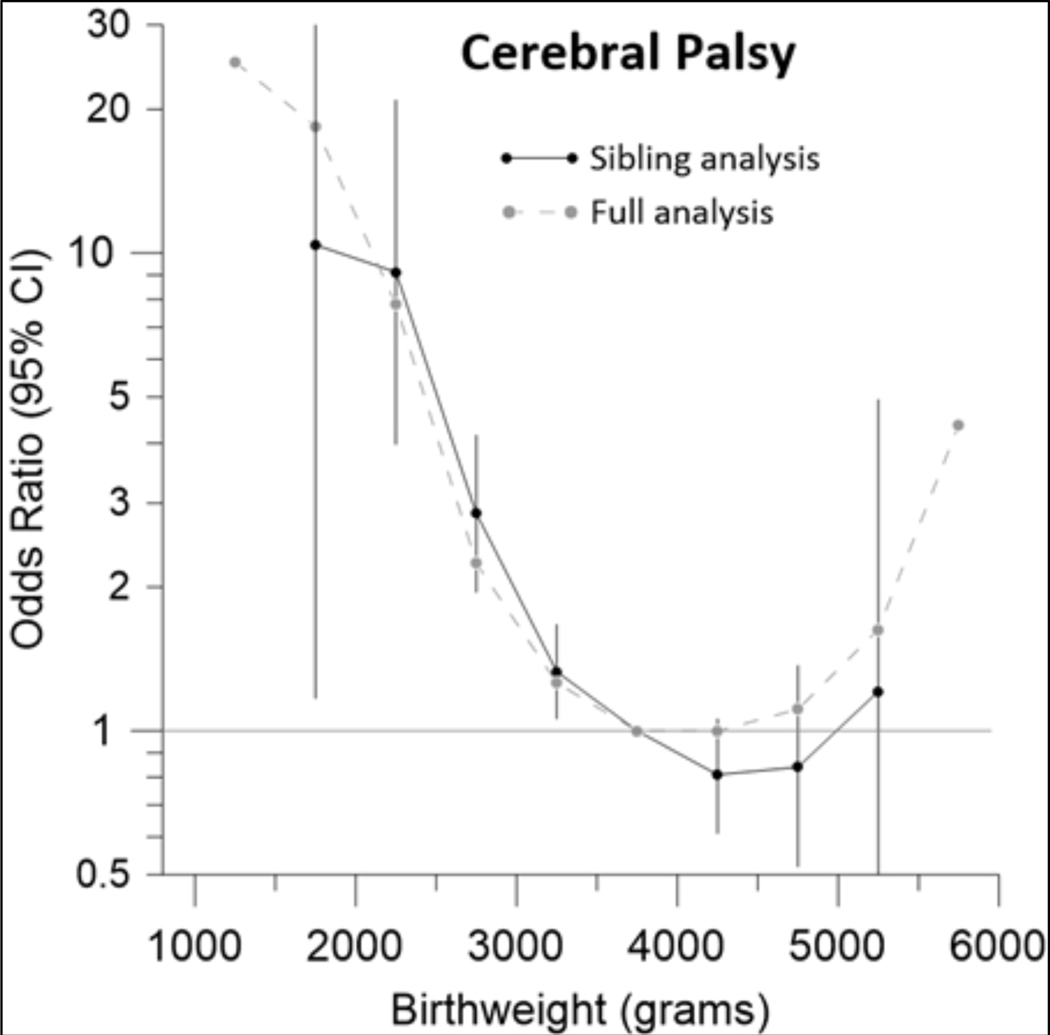
Results: The risk of neurodevelopmental disabilities at term steadily increased at birth weights lower than 3.5 kg. Using the category of 3.5-3.9 kg as the reference, the odds reached 25-fold for cerebral palsy at the smallest weights (95% confidence interval 8.0, 79), 16-fold for vision/hearing disability (4.0, 65), 11-fold for intellectual impairment (6.9, 17), 7-fold for schizophrenia (1.0, 50), 5.4-fold for epilepsy (2.6, 12), and 3.5-fold for autism spectrum (1.3, 9.4) and behavioral disorders including attention-deficit hyperactivity disorder (2.1, 5.4). Associations remained robust with sibling controls.
Conclusions: Reduced fetal growth is a powerful predictor of a wide variety of neurodevelopmental disabilities independent of preterm delivery.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures



References
-
- Moster D, Lie RT, Markestad T. Long-term medical and social consequences of preterm birth. N Engl J Med 2008; 359(3): 262–73. - PubMed
-
- Irgens LM. The Medical Birth Registry of Norway. Epidemiological research and surveillance throughout 30 years. Acta Obstet Gynecol Scand 2000; 79(6): 435–9. - PubMed
-
- Morken NH, Skjaerven R, Wilcox AJ. Ultrasound prediction of perinatal outcome: the unrecognised value of sibling data. BJOG 2015; 122(12): 1674–81. - PubMed
-
- Norwegian Ministry of Labour and Social Affairs. The Norwegian Social Insurance Scheme. January2020. https://www.regjeringen.no/contentassets/03b0e088c8f44a8793ed0c0781556b1... (accessed August 11, 2020.
-
- Moster D, Lie RT, Irgens LM, Bjerkedal T, Markestad T. The association of Apgar score with subsequent death and cerebral palsy: A population-based study in term infants. J Pediatr 2001; 138(6): 798–803. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
