

Adaptation of left ventricular diastolic function to pregnancy: a systematic review and meta-analysis
- PMID: 34001811
- PMCID: PMC8452327
- DOI: 10.1097/HJH.0000000000002886
Adaptation of left ventricular diastolic function to pregnancy: a systematic review and meta-analysis
Abstract
Objective: To meta-analytically determine the adaptation of left ventricular diastolic function (LVDF)-indices to singleton normotensive pregnancies.
Methods: Literature was retrieved from PubMed and Embase. We included studies that reported a nonpregnant reference measurement and LVDF indices (mitral inflow signals, left atrial volume and tissue Doppler measurements). Mean differences between pregnant and reference measurements and weighted means of absolute values were calculated using a random-effects model.
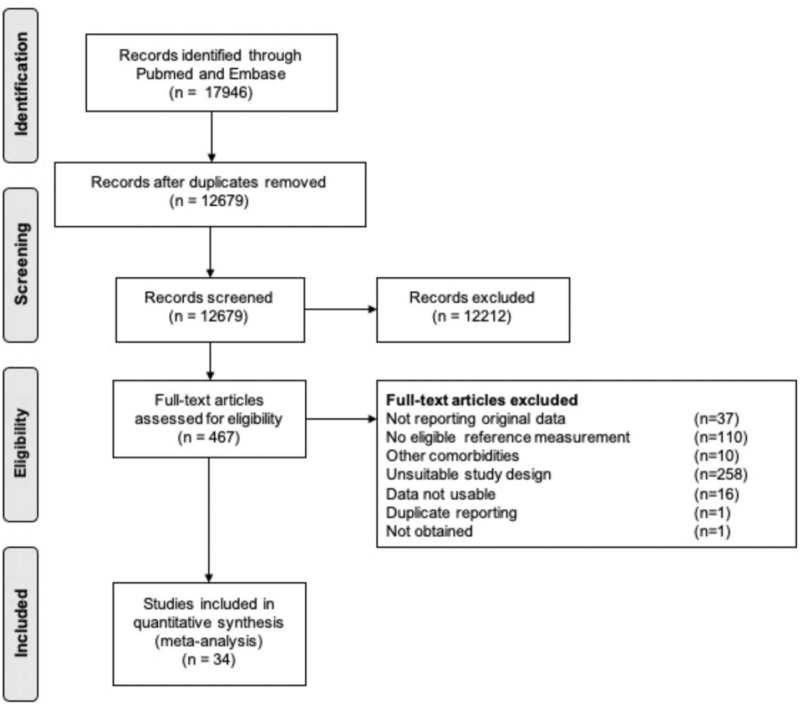
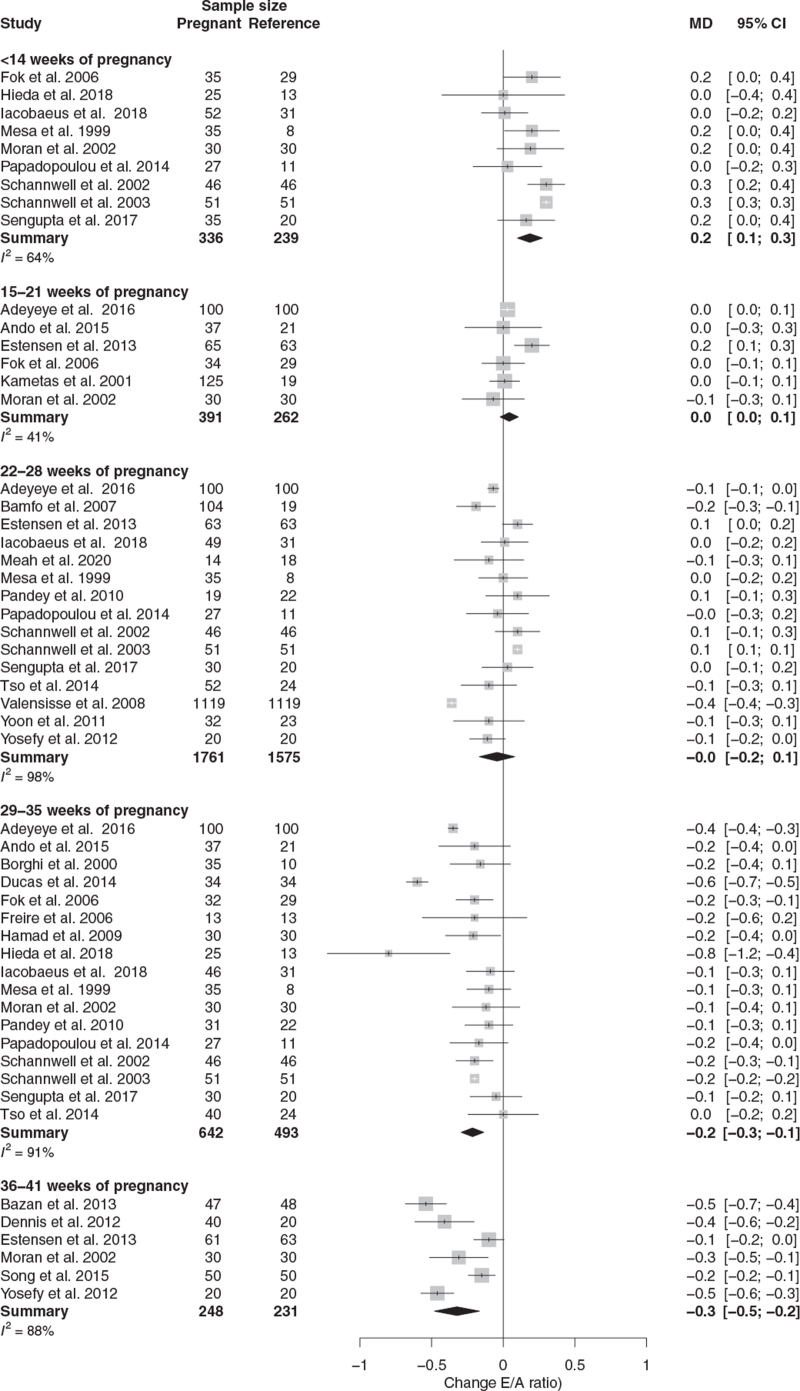
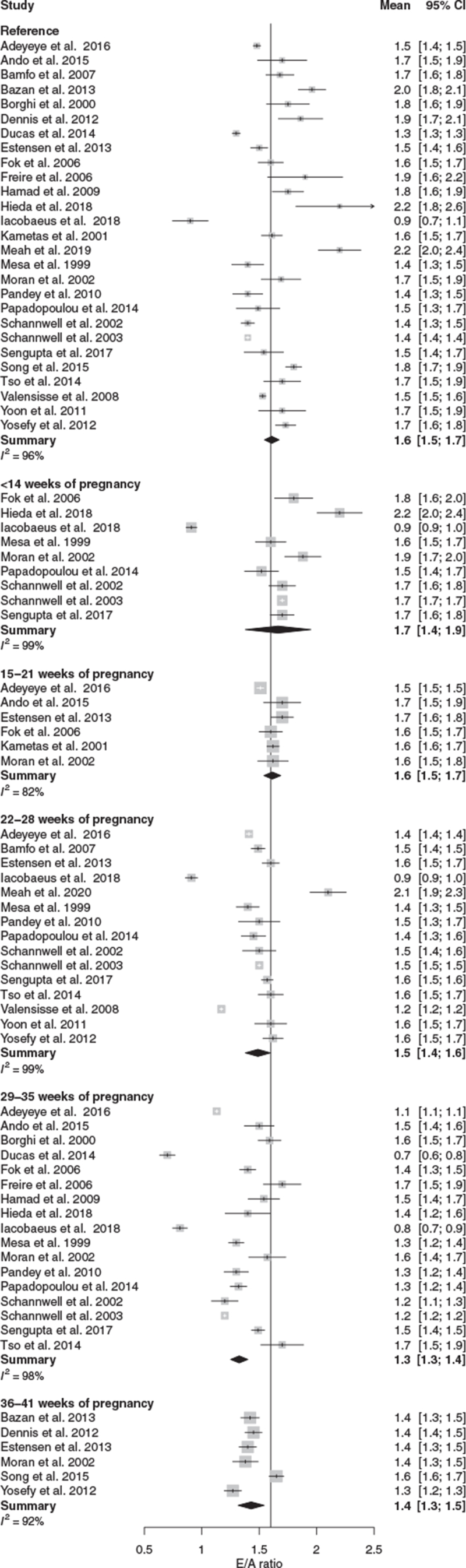
Results: We included 34 eligible studies. Normotensive pregnancies were characterized by an initially larger increase in the passive left ventricular filling (E-wave peak velocity, 13%) compared to active left ventricular filling during diastole (A-wave peak velocity, 6%) resulting in a 16% increase of the E/A ratio in the first trimester. The E/A ratio progressively decreased during advancing gestation to -18% at term, resulting from stabilizing E-wave peak velocity and increased A-wave peak velocity. The E/e' ratio was increased between 22 and 35 weeks (a maximal increase of 13%) in normotensive pregnancy. Left atrial volume (LAV) progressively increased from 15 weeks onwards with a maximal increase of 30% between 36 and 41 weeks.
Conclusion: LVDF in normotensive pregnancy was improved in the first trimester after which LVDF progressively worsened. Large-scale studies in normotensive and hypertensive complicated pregnancies are needed for a more precise insight into LVDF changes during pregnancy.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Meah VL, Cockcroft JR, Backx K, Shave R, Stöhr EJ. Cardiac output and related haemodynamics during pregnancy: a series of meta-analyses. Heart 2016; 102:518–526. - PubMed
-
- de Haas S, Ghossein-Doha C, van Kuijk SMJ, van Drongelen J, Spaanderman MEA. Physiological adaptation of maternal plasma volume during pregnancy: a systematic review and meta-analysis. Ultrasound Obstet Gynecol 2017; 49:177–187. - PubMed
-
- Duvekot JJ, Cheriex EC, Pieters FA, Menheere PP, Peeters LL. Early pregnancy changes in hemodynamics and volume homeostasis are consecutive adjustments triggered by a primary fall in systemic vascular tone. Am J Obstet Gynecol 1993; 169:1382–1392. - PubMed
-
- de Haas S, Ghossein-Doha C, Geerts L, van Kuijk SMJ, van Drongelen J, Spaanderman MEA. Cardiac remodelling during normotensive and hypertensive complicated pregnancies: a systematic review and meta-analysis. Ultrasound Obstet Gynecol 2017; 50:683–696. - PubMed
-
- Melchiorre K, Sharma R, Khalil A, Thilaganathan B. Maternal cardiovascular function in normal pregnancy. Hypertension 2016; 67:754–762. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
